Influence of Socio-Economic Factors on Contraceptive Use among Rural Women in Gwagwalada Area Council FCT, Abuja, Nigeria
-
Odera Chukwumaijem Okafor

Department of Geography, Faculty of Environmental Sciences, Alex Ekwueme Federal University Ndufu-Alike, Ebonyi, Nigeria
Ursula Ihechimere IkeokwuDepartment of Geography, Faculty of Environmental Sciences, Alex Ekwueme Federal University Ndufu-Alike, Ebonyi, Nigeria
| Received 21 Oct, 2023 |
Accepted 05 Feb, 2024 |
Published 14 Feb, 2024 |
Background and Objective: Contraception techniques have been practiced since antiquity, but efficient and safe methods were only made available in the twentieth century. The study examined the influence of socio-economic factors on contraceptive use among rural women in Gwagwalada Area Council, FCT, Abuja, Nigeria. Materials and Methods: A structured questionnaire was used to gather the study’s data. From the study area, 187 married women in total were chosen at random. Both descriptive and inferential statistics were used to analyze the data. Results: According to the results, 65% of the respondents thought birth control was helpful. The findings also revealed that the biggest barriers to using birth control were ignorance of its existence and religious beliefs. Additionally, 29.3% of respondents said they had never brought up birth control with their husbands. Additionally, it was discovered that 50.7% of the respondents thought that using birth control encouraged marital infidelity. The mainstream media did a bad job of disseminating information. Conclusion: The study advises primary health facilities to have the necessary tools to provide family planning services.
INTRODUCTION
Population refers to the total number of people living in a certain area, such as a town, city, state or country. Birth control is a critical socioeconomic issue. Overpopulation and rapid population increase continue to be major concerns for many national governments and the international community1-4. Numerous studies5,6 have linked high population growth rates, especially in the face of poor productivity to a variety of societal issues, from political instability to poverty, land scarcity, hunger and environmental degradation.
Many nations, including Korea, Brazil, Columbia, China, India, Bangladesh and Malawi, have effectively used family planning as a technique of limiting population growth to stop the problems associated with high population growth rates4,7-9.
In order to slow down the rapid rate of population growth that it is currently experiencing, Nigeria has also chosen family planning as a tactic. However, Izugbara et al.10 found that, this tactic or practice is still not widely accepted. Numerous studies have shown that despite the government’s efforts in this area, the adoption rate of contemporary birth-control services and facilities or family planning, in Nigeria is still virtually negligible10-12.
Nigeria’s government has taken a number of actions to address the population issue and its related issues. The creation of a national population policy, whose main goals are to alleviate the burden that high fertility and population growth rates continue to place on families’ health, standard of living, the nation’s agriculture and food supply, unemployment, educational opportunities and finite economic resources, is paramount among the measures.
Family planning, commonly referred to as birth control, is the deliberate use of contraceptive methods by a couple to restrict or space out the number of children they wish to have. Birth control is currently regarded as a fundamental right of individuals and couples to have as many children as they want, when they want them, with the fullest awareness of the implications of their choices and access to the means of carrying those choices through13.
Birth control is a style of thinking and living that is voluntarily embraced by people and couples on the basis of information, attitudes and responsible decision-making in order to advance the health and welfare of their family unit13.
In Nigeria, there are many different types of healthcare facilities, geopolitical regions and urban and rural settings14. These variations are explained by a number of supply and demand-related issues, which also contribute to Nigeria’s low rates of contraceptive usage and choice13.
Many Nigerian women prefer to have abortions to eliminate their unwanted pregnancies15. A lot of abortions are performed in dangerous settings because they are illegal in Nigeria (unless a doctor recommends it to save a mother’s life). These abortions have severe repercussions that frequently result in death and may even be life-threatening.
In Nigeria, abortion causes 20 to 40% of maternal fatalities16. According to the Do and Kurimoto14 findings, approximately 72% of women and 90% of men in Nigeria are aware of at least one form of contraception, whether it is a traditional approach or a modern one. Traditional procedures are less well-known than contemporary ones. Only 36% of women are familiar with the traditional method, compared to about 71% of women who are.
Only 5.1% of all women in the nation were using family planning, according to a 2000-2001 general household survey14, while the remaining 94.9% were not. However, from 2004 to 2012, there was a gradual rise in the use of contraceptives among women. This has made Nigeria’s population crisis, estimated at 140 million based on data from the 2006 census, worse14. In Nigeria, 85% of the severely poor resided in rural regions and two-thirds worked on farms17. Therefore, the purpose of this study is to investigate how socioeconomic factors influence rural women’s use of contraception in the Gwagwalada Area Council of the Federal Capital Territory, Abuja, Nigeria.
MATERIALS AND METHODS
Study area: One of the FCT’s six Area Councils in Abuja, Nigeria, is called Gwagwalada. The town in the area council, with a 1,043 km2 area, is also called Gwagwalada. The Gwagwalada Area Council is situated between Longitudes 7000'E and 7005'E and Latitudes 855'N and 9000'N. Its neighbours are the Kwali Area Council to the South, the Abuja Municipal Area Council to the North-East, the Kuje Area Council to the East, the Abaji Area Council to the West, the Kwali Area Council to the South and the Suleja Local Government Area of Niger State to the North18.
The study area is located in the tropical climate zone of the world. It has an average temperature of about 30-37°C yearly and a mean total annual rainfall of approximately 1,650 mm per annum19. Additionally, it is situated at the Usuma Dam Flood Plain on a low area of land in the Federal Capital Territory. Although it slopes downward, it is not completely flat. It has sedimentary rock and basement complex rock as its foundation, making some areas of it resistant to flooding and others vulnerable to erosion.
Site selection: On February 13th and 14th, 2018, a site was chosen so that researchers could become familiar with the study area. Out of the ten wards of Gwagwalada, five were randomly chosen for this survey: Dobi, Ibwa, Paiko, Ikwa and Gwako. To comprehend the nature of the study area and be aware of the many research methodologies, the varied effects of socioeconomic factors on contraceptives in the area were carefully and critically observed.
Data collection: Data from both primary and secondary sources were used. Journals and articles, both published and unpublished, are among the sources of secondary data. The primary data came from field research after a questionnaire was distributed. Field inquiry data were treated to both necessary inferential statistical procedures as well as descriptive statistical methods.
Sample frame: There were 157,770 people living in the Gwagwalada Area Council14. Zuba, Ibwa, Ikwa, Kutunku, Dobi, Paiko, Tungamaje, Gwako, Quarter and Central wards are the ten wards that makeup Gwagwalada. However, just five wards-Dobi, Ikwa, Ibwa, Paiko and Gwako-were chosen for the investigation. These communities were chosen because they were the only ones of the ten wards that were primarily rural. These five wards were deemed suitable for the study since it is based on rural women.
Sampling procedure and sample size: In this study, which selects various portions of the entire population, random sampling was used. Multi-stage sampling was the sampling method utilized to acquire the data. First, five of the ten wards-Zuba, Ibwa, Ikwa, Kutunku, Dobi, Paiko, Tungamaje, Gwako, Quarter and Central wards were chosen to be studied. Due to the fact that these are the ten wards in the Gwagwalada area council’s rural areas, the wards are chosen in the second stage using the purposive sampling method. The five wards that were chosen are Gwako, Paiko, Ikwa and Dobi. Multistage sample size technique19 was used in the third stage to determine the study area’s sample size:
Where:
| Z | = | Confidence level at 95% (1.96) | |
| P | = | Interval (0.4) | |
| d | = | Error 0.07 | |
| N | = | Sampling population | |
| n | = | 187.3 |
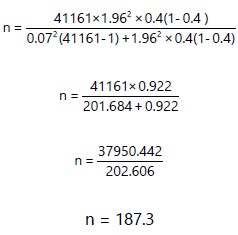 |
Approximately 187 to a whole number.
| Table 1: | Sample frame and sample size of selected wards | |||
| Selected wards | No. of settlement in selected wards | Selected settlements | Population of selected wards |
Sample size |
| Dobi | 11 |
Kaida sabo | 8712 |
34 |
| Wumi | ||||
| Kwalita | ||||
| Dobi | ||||
| Gwako | 7 |
Gwako | 9107 |
35 |
| Giri | ||||
| Malauni | ||||
| Kpasele | ||||
| Ibwa | 6 |
Ibwa sarki | 3502 |
37 |
| Dukwa | ||||
| Gurfata | ||||
| Ibwa sabo | ||||
| Ikwa | 4 |
Ikwa | 9582 |
39 |
| TunganLandan | ||||
| Chitimu | ||||
| Paiko | 8 |
Paiko sarki | 10258 |
42 |
| Katse | ||||
| Kaida isoho | ||||
| Passo | ||||
| Total | 36 |
41161 |
187 |
|
| Source: Researcher’s Intern, 2018 | ||||
Therefore, a sample size of 187 married women was randomly chosen from the research area’s population of 41161 for this study (Table 1).
Method of data analysis: The variables gathered from the field were analyzed in this study using descriptive statistics, including percentages, frequency distribution, tables and charts, as well as with the use of the Statistical Package for Social Science (VERSION 14.0). To construct the hypothesis, inferential statistics like the correlation coefficient were used.
RESULTS AND DISCUSSION
Socio-economic characteristics of respondents: Data on the respondents’ socioeconomic characteristics were gathered, analyzed and presented appropriately.
Age distribution of respondents: The information about the respondents’ age distribution displayed the age distribution of the research area’s respondents. It was discovered that 1.0% of respondents were under twenty, while 15.33% were between the ages of twenty and thirty. In addition, 65.33% of respondents were between the ages of 31 and 40, 13.33% were between the ages of 41 and 50 and the remaining 11.33% were over the age of 50. This indicates that respondents between the ages of 31 and 40 had a higher sample size than respondents in any other age frequency or age bracket in the study area. However, rural women between the ages of 20 and 45 who live in areas with high fecundity tend to use contraceptives more frequently. The age, education and wealth of the woman’s home are all taken into account in the modelling of contraceptive use. The usual set of exogenous variables in microeconomic models of human behaviour consists of these variables. Other variables like planned family size, age at marriage or parity are typically viewed as endogenous and are not included in the reduced form specification4.
Sex distribution of respondents: Table 2 displays the data on the distribution of sexes. Table 2 showed that 187 respondents (100%) were women. This suggested that only females were included in the study’s sample, as there was a lot of focus on how women perceived using contraceptives in the study location.
Distribution of respondent by marital status: According to the study, 88% of respondents were married, 6.7% had divorced and the remaining 5.3% had been widowed. As a result of the majority of respondents being married and having a high fertility rate, the population of the study area has increased.
| Table 2: | Sex distribution of respondents | |||
| Gender | Frequency |
Percentage |
| Male | 0 |
0 |
| Female | 187 |
100 |
| Total | 187 |
100 |
| Source: Researcher’s Intern, 2018 | ||
| Table 3: | Distribution of respondent by occupation | |||
| Status | Frequency |
Percentage |
| Civil servant | 50 |
26.7 |
| Business woman | 40 |
21.4 |
| Farmer | 85 |
42.5 |
| Student | 12 |
6.4 |
| Total | 187 |
100 |
| Source: Researcher’s Intern, 2018 | ||
Distribution of respondent by occupation: Table 3 displays the respondents’ occupations. As 42.5% of respondents were farmers, 21.4% were businesswomen, 26.7% were civil servants and the final twelve respondents (6.4%) were students. Since the majority of the respondents worked in agriculture, it is possible that they would have seen people from varied socioeconomic backgrounds. However, the study area has a high proportion of farming women, indicating that some of the women may not have access to information about using contraceptives.
Distribution of the respondents by religion: In the study area 26% of respondents practiced Christianity, 68% of respondents practiced Islam and 6% of respondents practiced traditional religion. This suggested that Muslims make up the majority of the local population in the study area. However, some religions accept having many wives; as a result, having more wives will likely result in having more offspring, which will increase population (vice-versa). It is sad that policymakers and program designers have not effectively tapped into religion to promote contraceptive usage in Northern Nigeria. Religion is essential to behavioral change20.
Distribution of respondents by number of children: The present study displays information on the distribution of respondents by the number of children. Each responder in the research area has a different number of kids, with variations including; in the study area, 6.67% of respondents had one child, 14.67% had two children, 20% had three children and 58.6% had four or more children. This suggests that the study area has a high fertility rate. According to the results, the majority of respondents had more than four kids.
Educational attainment of respondents: The present study displays the respondents’ educational attainment. The study also showed that 4.8% of respondents had completed their basic education, 54.8% had completed their secondary school, 21.6% had completed their tertiary education and 18.8% had not completed any formal education. It may be concluded that the study area has a moderately high literacy rate. Most of the responders had completed secondary school.
Since the majority of the respondents held secondary school diplomas, it was expected that they would learn about birth control methods in class, particularly in biology. Because it undermines traditional birth spacing practices like prolonged breastfeeding or postpartum abstinence without lowering fertility desires or raising the age at marriage. Cohen4 reported that small amounts of education have occasionally been found to rise rather than lower fertility. Furthermore, women with higher levels of education are less likely to view family planning as a death sentence and are more likely to be aware of other family planning options and their possible drawbacks.
| Table 4: | Income level of respondents in the study area | |||
| Income (₦) | Frequency |
Percentage |
| Below 8,000 | 35 |
18.7 |
| 8,000-15,000 | 50 |
26.7 |
| 15,000-23,000 | 40 |
21.4 |
| 23,000-30,000 | 42 |
22.5 |
| Above 30,000 | 20 |
10.7 |
| Total | 187 |
100 |
| Source: Researcher’s Intern, 2018 | ||
Distribution of respondents by income level: Table 4 displays the information on the distribution of respondents by income level. According to the table, 18.7% of respondents made less than ₦80000; 26.7% made between ₦8000 and ₦15000 and 21.4% made between ₦15000 and ₦23000: While the remaining 10.7% of respondents earned more than ₦30,000; 22.5% of respondents made between ₦23,000 and ₦30,000. Fewer respondents have high incomes, which suggest that access to money would be a barrier to birth control use in the research location.
Knowledge of birth control in the study area: It displays information on birth control knowledge. About 60% of respondents said they were aware of birth control, whereas 40% said they were unaware of its applications. This shows that respondents with less understanding of birth control applications have larger families than respondents with more information.
Source of information concerning birth control: It displays the data on the sources of birth control-related information. According to the results, 28% of respondents learned about birth control via friends, 22.67% from the media, 40% from health professionals and the remaining 9.33% learned about it from other sources. This suggested that it is important to stress the roles played by the media and health professionals in promoting birth control in the research area.
Birth control practice: The study displays the information on the respondents’ distribution by method of birth control. Ninety respondents (48.13%) adopted birth control, whereas the other ninety-seven respondents (51.87%) did not use any birth control, according to the diagram. Given that the majority of respondents said they did not use birth control, which also led to an increase in population, it follows that the fertility rate in the study area is likely to increase in the years to come. A number of doors have opened for Nigeria to duplicate the Algerian experience, but they have not yet been taken advantage of. One of these is described in a report of esteemed scholars who met to discuss "reproductive health issues in Nigeria" from an Islamic perspective and issued a fatwa for the termination of life-threatening pregnancies21.
Hindrance to birth control: Birth control is allegedly not used effectively in the nation due to several obstacles. The 34% of respondents claimed it was because of religion, 24.67% claimed it was because of custom and 41.33% claimed it was because of ignorance. Given that many respondents said that lack of information is the main barrier to the use of birth control in the study areas, it follows that additional efforts should be made to raise awareness in those communities.
Perception of birth control: The perceptions of respondents regarding the value of birth control were gathered and shown in Table 5. The 40.1% of respondents thought it was helpful, compared to 34.8% who thought it wasn’t helpful and 25.1% who weren’t sure. Birth control is presumably widely accepted in the study because the majority of respondents saw it as beneficial.
| Table 5: | Perception of birth control | |||
| Variables | Frequency |
Percentage |
| Beneficial | 75 |
40.1 |
| Not beneficial | 65 |
34.8 |
| Not sure | 47 |
25.1 |
| Total | 187 |
100 |
| Source: Researcher’s Intern, 2018 | ||
| Table 6: | Respondents’ view on ideal time to adopt birth control | |||
| Variables | Frequency |
Percentage |
| As soon as marriage is contracted | 0 |
0 |
| After the couple has at least one child | 42 |
23 |
| After the birth of each child | 55 |
29 |
| After the couple have had all the children they want to have | 90 |
48 |
| Total | 187 |
100 |
| Source: Researcher’s Intern, 2018 | ||
Respondents’ view on ideal time to adopt birth control: The opinions of the respondents on the best time to start using birth control were gathered, analyzed and shown in Table 6. In accordance with 23% of respondents, couples should adopt birth control after having at least one kid, 29% after each child and 48% after having all of the children they intend to have. This suggested that the respondents thought contraception should be used after couples have all the kids they want. This has the consequence that other benefits of birth control are still unknown in the study area.
Methods of birth control: It depicts the technique of birth control that is most common in the study location. As 60% of respondents said they used birth control pills, 20% said they used injections, 10% said they used surgery and 10% said they utilized conventional methods. This suggests that the pill-based birth control approach is still widely used in the area. Encouragement of a more dependable injection approach is necessary. However, the opportunity for concealment during the usage of tablets has frequently been cited as the reason why they are preferred in Sub-Saharan Africa (SSA) over other contraceptives22-24.
Hypothesis testing: The study’s hypothesis was tested using multiple regression analysis.
Ho = There is no significant relationship between income level, education, religion, occupation and contraceptive use
The model summary between the use of contraceptives and the respondents’ socioeconomic characteristics. The coefficient of regression (0.309) showed that the respondents’ wealth, educational position, religion and occupation all had an impact on 30.9% of their use of contraceptives. Other factors, including respondents’ ages, marital statuses, household sizes, access to contraceptives, social pressure and availability of contraceptives, among others, account for 69.1% of the respondents’ usage of contraceptives.
The relationship between the analyzed socioeconomic characteristics and respondents’ use of contraceptives is shown in Table 7. Contraceptive use in the area increases by 7 and 1.8% for every 1% rise in respondents’ levels of education and religious affiliation, respectively, while it decreases by 1.9 and 2.9% for every 1% decrease in respondents’ income and occupation.
There is a need for a big awareness effort to be undertaken about the dangers of expanding population and increasing family sizes. This will help supplement the low literacy level among individuals.
The media should also be responsible for disseminating information regarding the relevance and timeliness of birth control.
| Table 7: | Relationship between socioeconomic variables and contraceptives | |||
Unstandardized coefficients |
|||||
| Model | B |
Standard error |
Standardized coefficients beta |
t |
Sig. |
| Constant | 1.346 |
0.208 |
6.469 |
0 |
|
| Income | -0.019 |
0.029 |
-0.048 |
-0.642 |
0.522 |
| Education | 0.071 |
0.032 |
0.161 |
2.21 |
0.028 |
| Religion | 0.018 |
0.048 |
-0.029 |
-0.381 |
0.704 |
| Occupation | -0.029 |
0.039 |
-0.055 |
-0.743 |
0.459 |
| Dependent Variable: Contraceptive, Source: Researcher’s Intern, 2018 | |||||
Establishing primary health facilities in rural locations can improve access to healthcare services. Local individuals are hired at such health centres, allowing people to interact freely with one another. This study is extremely important in many ways, thus its value extends beyond the course or field alone. Different authorities at various tiers can use it as a tool to manage population increase, promote economic growth and raise people’s standards of life.
Also, individuals, the government and society as a whole will gain greatly from the study since the findings will give health service providers the information they need to improve their family planning awareness campaigns. In addition, the study will raise awareness of the negative, socio-economic and cultural beliefs about the use of birth control. The main and only limitation of the study was the lack of funding.
CONCLUSION
According to the study, a large proportion of respondents accepted birth control measures as being helpful. Also, it was discovered that the main barriers to birth control use in the study area were a lack of knowledge of their existence and religious beliefs. Additionally, it was discovered that a great number of the respondents thought that using birth control encouraged marital infidelity. Also, the media, which is meant to be a key source of information regarding this topic, has not been active.
SIGNIFICANCE STATEMENT
The purpose of the study was to find out the influence of socio-economic factors on contraceptive use among women in the study area. The set objectives were to examine the prevalence of contraceptives, know the knowledge of contraceptive use among rural women and find out the attitudes of rural women towards contraceptive use in the study area. The study discovered that a lack of knowledge of existence of birth control and religious beliefs posed a greater barrier. Also, a great number of the respondents thought that using birth control encouraged marital infidelity. The study will be of great benefit to individuals, the government and society as a whole because the findings would equip health service providers in the study area.
REFERENCES
- Lucas, D., 1992. Fertility and family planning in Southern and Central Africa. Stud. Fam. Plann., 23: 145-158.
- Oliver, R., 1995. Contraceptive Use in Ghana: The Role of Service Availability, Quality, and Price. World Bank Publications, Washington, DC, ISBN: 9780821330203, Pages: 46.
- Adebowale, S.A., I.A. Adeoye and M.E. Palamuleni, 2013. Contraceptive use among Nigerian women with no fertility intention: Interaction amid potential causative factors. Afr. Popul. Stud., 27: 127-139.
- Cohen, B., 2000. Family planning programs, socioeconomic characteristics, and contraceptive use in Malawi. World Dev., 28: 843-860.
- Caldwell, J.C. and P. Caldwell, 1977. The role of marital sexual abstinence in determining fertility: A study of the Yoruba in Nigeria. Popul. Stud., 31: 193-217.
- Chikovore, J., G. Lindmark, L. Nystrom, M.T. Mbizvo and B.M. Ahlberg, 2002. The hide-and-seek game: Men's perspectives on abortion and contraceptive use within marriage in a rural community in Zimbabwe. J. Biosoc. Sci., 34: 317-332.
- Nag, M., 1992. Family Planning Success Stories in Bangladesh and India. World Bank Publications, Washington, DC, Pages: 37.
- Duze, M.C. and I.Z. Mohammed, 2006. Male knowledge, attitudes, and family planning practices in Northern Nigeria. Afr. J. Reprod. Health, 10: 53-65.
- Gule, G., 1994. Socio-cultural constraints to family planning in Swaziland. Can. Stud. Popul., 21: 35-49.
- Izugbara, C., L. Ibisomi, A.C. Ezeh and M. Mandara, 2010. Gendered interests and poor spousal contraceptive communication in Islamic Northern Nigeria. BMJ Sex. Reprod. Health, 36: 219-224.
- Omo-Aghoja, L.O., V.W. Omo-Aghoja, C.O. Aghoja, F.E. Okonofua and O. Aghedo et al., 2009. Factors associated with the knowledge, practice and perceptions of contraception in rural Southern Nigeria. Ghana Med. J., 43: 115-121.
- Jayaraman, A., V. Mishra and F. Arnold, 2009. The relationship of family size and composition to fertility desires, contraceptive adoption and method choice in South Asia. Int. Perspect. Sex. Reprod. Health, 35: 29-38.
- Monjok, E., A. Smesny, J.E. Ekabua and E.J. Essien, 2010. Contraceptive practices in Nigeria: Literature review and recommendation for future policy decisions. Open Access J. Contraception, 1: 9-22.
- Do, M. and N. Kurimoto, 2012. Women’s empowerment and choice of contraceptive methods in selected African countries. Int. Perspect. Sex. Reprod. Health, 38: 23-33.
- Otoide, V.O., F. Oronsaye and F.E. Okonofua, 2001. Why Nigerian adolescents seek abortion rather than contraception: Evidence from focus-group discussions. Int. Fam. Plann. Perspect., 27: 77-81.
- Oriji, V.K., I. Jeremiah and T. Kasso, 2009. Induced abortionamongst undergraduate students of University of Port Harcourt. Niger. J. Med., 18: 199-202.
- Abiodun, O.M. and O.R. Balogun, 2009. Sexual activity and contraceptive use among young female students of tertiary educational institutions in Ilorin, Nigeria. Contraception, 79: 146-149.
- Balogun, O. and O.Y. Balogun, 2001. The Federal Capital Territory of Nigeria: A Geography of its Development. Ibadan University Press, Ibadan, Nigeria, ISBN-13: 9789781213939, Pages: 230.
- Ndep, A.O., 2014. Informed community participation is essential to reducing maternal mortality in Nigeria. Int. J. Health Psychol. Res., 2: 26-33.
- Shrestha, S., 2002. Increasing contraceptive acceptance through empowerment of female community health volunteers in rural Nepal. J. Health Popul. Nutr., 20: 156-165.
- Odimegwu, C.O., M. Ojo and A. Siyagande, 1997. Regional correlates of choice of contraceptive methods in Nigeria. Korea J. Popul. Dev., 26: 131-145.
- Sule, S.T., H.S. Umar and N.H. Madugu, 2006. Knowledge and use of modern contraception among Muslim women in Zaria, Nigeria. J. Islamic Med. Assoc. North Am., 38: 10-16.
- Mandara, M., 2012. Family planning in Nigeria and prospects for the future. Int. J. Gynecology Obstet., 117: 1-4.
- Nwachukwu, I. and O.O. Obasi, 2008. Use of modern birth control methods among rural communities in Imo State, Nigeria. Afr. J. Reprod. Health, 12: 101-108.
How to Cite this paper?
APA-7 Style
Okafor,
O.C., Ikeokwu,
U.I. (2024). Influence of Socio-Economic Factors on Contraceptive Use among Rural Women in Gwagwalada Area Council FCT, Abuja, Nigeria. Asian Science Bulletin, 2(1), 1-9. https://doi.org/10.3923/asb.2024.01.09
ACS Style
Okafor,
O.C.; Ikeokwu,
U.I. Influence of Socio-Economic Factors on Contraceptive Use among Rural Women in Gwagwalada Area Council FCT, Abuja, Nigeria. Asian Sci. Bul 2024, 2, 1-9. https://doi.org/10.3923/asb.2024.01.09
AMA Style
Okafor
OC, Ikeokwu
UI. Influence of Socio-Economic Factors on Contraceptive Use among Rural Women in Gwagwalada Area Council FCT, Abuja, Nigeria. Asian Science Bulletin. 2024; 2(1): 1-9. https://doi.org/10.3923/asb.2024.01.09
Chicago/Turabian Style
Okafor, Odera, Chukwumaijem, and Ursula Ihechimere Ikeokwu.
2024. "Influence of Socio-Economic Factors on Contraceptive Use among Rural Women in Gwagwalada Area Council FCT, Abuja, Nigeria" Asian Science Bulletin 2, no. 1: 1-9. https://doi.org/10.3923/asb.2024.01.09

This work is licensed under a Creative Commons Attribution 4.0 International License.