Risk Factors Associated with Urinary Schistosomiasis and its Spatial Distribution Among Almajirai in Selected Localities in Katsina State, Nigeria
-
Hafsat Sada Rufai


Department of Biological Sciences, Federal University Dutsin-Ma, Katsina State, Nigeria
Timothy AutaDepartment of Biological Sciences, Federal University Dutsin-Ma, Katsina State, Nigeria
James Bemshima OrpinDepartment of Biological Sciences, Federal University Dutsin-Ma, Katsina State, Nigeria
Emmanuel Dayo AlabiDepartment of Microbiology, Federal University Dutsin-Ma, Katsina State, Nigeria
| Received 16 Oct, 2024 |
Accepted 11 Jan, 2025 |
Published 30 Mar, 2025 |
Background and Objective: Urinary schistosomiasis is endemic to Nigeria and is attributable to poverty, particularly in resource-constrained populations. This study assessed the prevalence and risk factors of urinary schistosomiasis among Almajirai in Tsangaya schools (TS) in Safana, Dutsin-Ma and Kurfi Towns of Katsina State, Nigeria. Materials and Methods: This cross-sectional study was conducted across thirteen TS from June to September, 2023. Urine samples were tested for the ova of Schistosoma haematobium using the centrifugation technique and generated datasets were analyzed using SPSS (p<0.05) and Chi-square tests to test for association. Results: Of the 514 samples examined from 13 TS, 35.6% (183/514) were positive for the ova of S. haematobium. Dutsin-Ma Town had the highest prevalence of 46.5% (80/172) among the three municipalities studied. In comparison, the 16-20 years age group had the highest prevalence of 40.5% (15/37) among the age groups and the highest prevalence among the TS surveyed occurred in Mallam Hamza TS (60.7%). In contrast, Mallam Audu TS had the lowest prevalence (6.9%). Those in contact with large water bodies had a prevalence of 36.3% (127/350) and participants with hematuria recorded a higher prevalence (49.7%) than those who never passed blood in urine (17.1%). Predisposing risk factors for infection included age group (χ = 50.6220, p = 0.0000) and was significantly associated with hematuria (χ= 58.2460, p = 0.0000). Conclusion: The study localities were classified as moderate-risk areas (<50) for urinary schistosomiasis. Risk factors included contact with water bodies, age and lack of prior praziquantel treatment. To prevent further transmission, improved environmental sanitation, Almajirai’s mass deworming programs, access to clean water and public education on disease prevention and hygiene are recommended.
INTRODUCTION
Schistosomiasis (bilharziasis) is a significant tropical disease that has been neglected. It is second to malaria in terms of parasite-induced morbidity and mortality1. Schistosomiasis can occur as an acute or chronic parasitic disease. It is endemic to many developing countries in tropical and sub-tropical Africa, the Middle East, Asia and Latin America. Approximately 90% of the global burden of schistosomiasis is found in sub-Saharan Africa2. Agents of schistosomiasis are digenic blood flukes (trematode worms) belonging to the genus Schistosoma3. This neglected infectious disease is attributable to poverty and is endemic in resource-constrained regions. Water bodies contaminated with cercariae from Bulinus snails (the intermediate host) serve as a medium for human infection when they penetrate the unbroken skin. The larvae develop into adult Schistosomes and migrate to the vesical and pelvic venous plexuses, where the female Schistosomes lay eggs in the urinary bladder and ureters. This condition leads to the formation of ulcers and symptoms of urinary tract infection due to the accumulation of eggs in bladder tissues4. The infection is characterized by bloody urine (hematuria), bladder lesions, kidney failure and bladder cancer5.
The Almajirai education system has been a longstanding tradition among Muslims in Northern Nigeria and neighboring countries. The Almajirai (pupil/student) are sent to a Mallam (teacher) to learn the Quran in Tsangaya schools (TS), where they reside separately from their families and attend TS on a full-time basis. Often, they lack basic resources and support from their teachers, leaving them vulnerable and having to fend for themselves from a young age. This self-sustaining lifestyle typically begins between 5 and 19 years of age2,6. Approximately 236 million people are infected with S. haematobium globally, with an estimated 140 million newly infected people annually, according to the World Health Organization (WHO), most new cases occur in underprivileged rural areas of Sub-Saharan Africa7.
In contrast, public health control measures to contain urinary schistosomiasis have been effectively implemented in countries such as China, Brazil, Egypt and Japan8. However, despite numerous attempts to reduce the national burden of urinary schistosomiasis in Nigeria through school-based interventions, the region has remained a significant hotspot in the global schistosomiasis crisis. This is due to the paucity of comprehensive data regarding the geographical spread of the disease, necessitating the need to determine its current prevalence in various localities to develop and recommend appropriate control measures9. Thus, this study was conducted to determine the risk factors and current prevalence rate of urinary bilharziasis among Almajirai in the towns of Dutsin-Ma, Kurfi and Safana in Katsina State, Nigeria.
MATERIALS AND METHODS
Study areas: The study was conducted in the towns of Safana, Dutsin-Ma, Kurfi, Katsina State, Nigeria. The three towns are situated in Safana, Dutsin-Ma and Kurfi Local Government Areas (LGAs) in the Western Region of Katsina State, Nigeria.
Study design and population: This study used a randomized cluster design and a cross-sectional approach for random urine sampling from Almajirai between June and September, 2023.
Sample size determination: The sample size for the study was determined using the single-proportion formula, assuming a 21.3% proportion of urinary schistosomiasis from a previous study conducted by Auta et al.2. A 95% confidence level and 5% precision were used. The single proportion formula used is:
where, n is the sample size, Z is the alpha risk represented in the z-score, P is the predicted prevalence and d is the absolute precision.
After the calculation, 514 participants were selected using random sampling. The participants were from Mallam Ishaq TS, Mallam Shuaibu TS, Mallam Audu TS, Mallam Abdulmajid TS, Mallam Ibrahim TS, Mallam Lawal TS, Mallam Hashimu TS, Mallam Aminu TS, Mallam Isa TS, Mallam Hamza TS, Mallam Abdulkarim TS, Mallam Abdullahi TS and Mallam Mustapha TS, respectively.
Data collection
Questionnaire survey: Structured questionnaires were administered to the participants and questions were asked regarding their sex, age, origin, parents’ occupation, educational background and contact with water bodies, etc.
Urine sample collection: Each participant was provided with a clean universal bottle labeled with their name and code. They were required to fill the bottle with urine between 10:00 am and 2:00 pm, as this was the optimal time to detect the presence of ova in urine due to the circadian rhythm of the parasite. The collected samples were placed in dark polyethylene bags kept cool in ice-packed containers and transported to the Biology Laboratory at the Federal University Dutsin-Ma for further analysis.
Ethical statement: The study protocol was reviewed and approved by the State Ministry of Health Ethical Clearance Committee in Katsina State under the approval number MOH/ADM/SUB/1152/1/555. Informed consent was obtained from the guardians (Mallams) of Almajirai, who were selected for the study. Those who did not consent or were unwilling to participate were excluded from the study. Participants were also given the freedom to withdraw from the study at any time.
Urine microscopy: To examine the urine samples for S. haematobium eggs, the samples were mixed and 10 mL of each sample was transferred to a clean centrifuge tube and spun at 1500 rpm for 5 min using a C2 series Centurion Scientific Centrifuge (Sussex, United Kingdom). The resulting sediment was examined under a compound (binocular) microscope (Motic Wetzlar, Germany) using a x10 objective lens. The presence of S. haematobium ova was confirmed by identifying their distinctive terminal spines using a 40x objective lens10.
Statistical analysis: The statistical Package for Social Science (SPSS) software was used to analyze the data. The Chi-square test and odds ratio at 95% confidence interval (CI) were used to measure the strength of association between variables. Values were considered statistically significant at a 95% confidence interval (CI) and a p<0.05.
RESULTS
Among the participants examined, 172 (33.5%) were from Dutsin-Ma, 65 (12.6%) from Kurfi and 277 (53.9%) from Safana Town. The prevalence of S. haematobium infection across the study localities was 35.6%. Dutsin-Ma Town had the highest prevalence at 46.5%, followed by Safana at 31.4% and Kurfi with the lowest prevalence of 24.6% (Table 1).
Within the Tsangaya schools (TS) surveyed, Mallam Hamza TS recorded the highest prevalence (60.7%), while Mallam Audu TS had the lowest prevalence (6.9%) (Table 2).
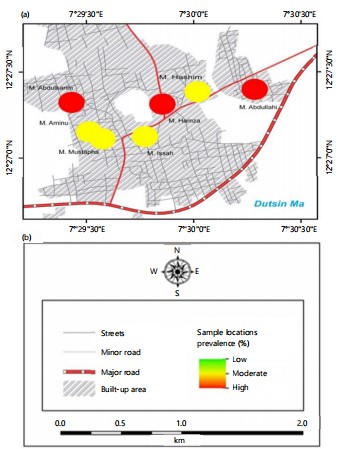
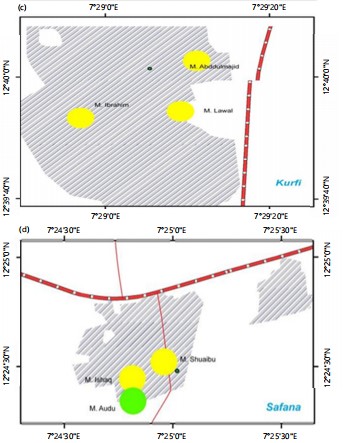
Regarding the spatial distribution of infection intensity, Mallam Hamza, Mallam Abdullahi and Mallam Abdulkarim TS in Dutsin-Ma Town recorded the highest prevalence rates of 60.7, 58.3 and 57.7%, respectively (Fig. 1a-d).
| Table 1: | Prevalence of Urinary schistosomiasis among Almajirai in Dutsin-Ma, Kurfi and Safana Towns | |||
| Study area | Number of samples examined | Number of sample positive | Prevalence (%) |
| Dutsin-Ma | 172 | 80 | 46.5 |
| Kurfi | 65 | 16 | 24.6 |
| Safana | 277 | 87 | 31.4 |
| Total | 514 | 183 | 35.6 |
| χ2 | 14.4760 | ||
| p-value | 0.0010 | ||
| χ2: Chi-squared test | |||
| Table 2: | Prevalence of urinary schistosomiasis among Almajirais schools in Dutsin-Ma, Kurfi and Safana Towns | |||
| School | Number of samples examined | Number of sample positive | Prevalence (%) |
| Mallam Ishaq TS | 180 | 75 | 41.6 |
| Mallam Shuaibu TS | 68 | 10 | 14.7 |
| Mallam Audu TS | 29 | 2 | 6.9 |
| Mallam Abdulmajid TS | 8 | 1 | 12.5 |
| Mallam Ibrahim TS | 35 | 6 | 17.1 |
| Mallam Lawal TS | 22 | 9 | 40.9 |
| Mallam Hashimu TS | 39 | 14 | 14.4 |
| Mallam Aminu TS | 23 | 10 | 43.5 |
| Mallam Isa TS | 28 | 10 | 35.7 |
| Mallam Hamza TS | 28 | 17 | 60.7 |
| Mallam Abdulkarim TS | 26 | 15 | 57.7 |
| Mallam Abdullahi TS | 12 | 7 | 58.3 |
| Mallam Mustapha TS | 16 | 7 | 43.8 |
| Total | 514 | 183 | 35.6 |
| χ2 | 50.6220 | ||
| p-value | 0.0000 | ||
| TS: Tsangaya school and χ2: Chi-squared test | |||
These schools were classified as high-risk schools among those studied, indicating a higher intensity of infection in these areas compared to others (Fig. 1a). Furthermore, all the schools surveyed in Kurfi Town were categorized as moderate-risk schools (Fig. 1c). In contrast, the schools surveyed in Safana Town included two moderate-risk schools and one low-risk school for infections (Fig. 1d). The findings reveal that the prevalence of positive samples varies by water source, with streams showing the highest prevalence (40.0%), followed by rivers (36.3%) and other sources (34.9%). Contact with water bodies did not significantly influence prevalence, with rates being similar for individuals in contact (35.8%) and those not in contact (34.7%). However, the type of water body was significantly associated with prevalence (p = 0.000), with dams having the highest rate (48.7%) compared to rivers (30.9%). Regarding the purpose of the visit, bathing and playing showed the highest prevalence (39.8%), but this association was not statistically significant (p = 0.102) (Table 3).
Regarding age, the group aged 16-20 years had the highest prevalence (40.5%), while the 6-10 years age group had the lowest prevalence (29.8%) (Table 4).
Additionally, the study found a significantly higher prevalence of blood in urine among participants reporting its presence (49.7%) compared to those without (17.1%) (χ2 = 58.246, p = 0.0000). History of praziquantel treatment did not significantly affect prevalence (χ2 = 0.916, p = 0.338), with similar rates observed in treated (40.2%) and untreated (34.7%) individuals. Time since the last praziquantel treatment also showed no significant association with prevalence (χ2 = 4.520, p = 0.340), though the highest prevalence was noted among individuals treated one month prior (60.0%) (Table 5).
|
| Table 3: | Risk factors associated with the prevalence of urinary schistosomiasis among Almajirai in Dutsin-Ma, Kurfi and Safana Towns | |||
| Source of water | Number of samples examined | Number of samples positive | Prevalence (%) |
| Well | 11 | 3 | 27.3 |
| Tap | 4 | 0 | 0.0 |
| River | 350 | 127 | 36.3 |
| Stream | 20 | 8 | 40.0 |
| Others | 129 | 45 | 34.9 |
| χ2 | 2.8130 | ||
| p-value | 0.5900 | ||
| Contact with water body | |||
| Yes | 416 | 149 | 35.8 |
| No | 98 | 34 | 34.7 |
| χ2 | 0.206 | ||
| p-value | 0.65 | ||
| Type of water body | |||
| River | 301 | 93 | 30.9 |
| Dam | 115 | 56 | 48.7 |
| Not applicable | 98 | 34 | 34.7 |
| χ2 | 25.6160 | ||
| p-value | 0.0000 | ||
| Purpose of visit | |||
| Bathing and playing | 299 | 119 | 39.8 |
| Fetching water | 107 | 28 | 26.2 |
| Fishing | 9 | 2 | 22.2 |
| Others | 1 | 0 | 0.0 |
| Not applicable | 98 | 34 | 34.7 |
| χ2 | 7.7420 | ||
| p-value | 0.1020 | ||
| χ2: Chi-squared test | |||
| Table 4: | Prevalence of urinary schistosomiasis among age groups | |||
| Age (years) | Number of samples examined | Number of samples positive | Prevalence (%) |
| 01-May | 16 | 5 | 31.3 |
| 06-Oct | 171 | 51 | 29.8 |
| Nov-15 | 290 | 112 | 38.6 |
| 16-20 | 37 | 15 | 40.5 |
| χ2 | 4.1680 | ||
| p-value | 0.2440 | ||
| χ2: Chi-squared test | |||
| Table 5: | Hematuria, history of praziquantel treatment and Urinary schistosomiasis among Almajirai in Dutsin-Ma, Kurfi and Safana Towns | |||
| Blood in urine | Number examined | Number positive | Prevalence (%) |
| Yes | 292 | 145 | 49.7 |
| No | 222 | 38 | 17.1 |
| χ2 | 58.246 | ||
| p-value | 0.0000 | ||
| Praziquantel history | |||
| Yes | 82 | 33 | 40.2 |
| No | 432 | 150 | 34.7 |
| χ2 | 0..9160 | ||
| p-value | 0.3380 | ||
| When last (Months) | |||
| 1 | 5 | 3 | 60.0 |
| 2 | 6 | 1 | 16.7 |
| 6 | 9 | 3 | 33.3 |
| Can’t remember | 61 | 27 | 44.3 |
| Not applicable | 433 | 149 | 34.4 |
| χ2 | 4.5200 | ||
| p-value | 0.3400 | ||
| χ2: Chi-squared test | |||
DISCUSSION
Almajirai are a vulnerable subset of the population and can serve as a reservoir for parasitic diseases, including urinary schistosomiasis. This underscores the need to assess the prevalence of the disease among this group to develop and recommend effective control measures. The overall prevalence of urinary bilharziasis among Almajirai in this study was 35.6% (183/514). The prevalence rate across the study localities fell within the moderate-risk range (<50) based on the national prevalence range of Nigeria11. The occurrence of urinary schistosomiasis in this study corroborates previous findings from studies conducted in Katsina, Sokoto and Jigawa States in Northwest Nigeria as well as in Takum, Northeast Nigeria2,9,12,13.
In comparison, infection with S. haematobium was more prevalent in Dutsin-Ma Town (46.5 %) than in Safana (31.4%) and Kurfi Town (24.6%) (Table 1). Furthermore, the current prevalence of urinary schistosomiasis in Dutsin-Ma is higher than that reported in previous studies among primary and secondary school students in the area14,15. We speculate that the increasing prevalence of S. haematobium infection in Dutsin-Ma Town may be attributable to the higher number of large water bodies in the area compared to other study localities (Fig. 1a). Consequently, Mallam Hamza, Mallam Abdullahi and Mallam Abdulkarim TS in Dutsin-Ma Town recorded the highest prevalence of infection at 60.7, 58.3 and 57.7%, respectively, classifying these TS as high-risk schools among those studied, while Mallam Audu TS in Safana Town recorded the lowest (6.9%) prevalence (Table 2). All surveyed schools in Kurfi Town were categorized as having a moderate risk of infection, suggesting a uniform risk level across the area (Fig. 1c). In contrast, the schools in Safana Town exhibited variability, with two classified as moderate-risk and one as low-risk, reflecting a mixed risk profile for infections in this locality (Fig. 1d).
Risk factors analyzed for S. haematobium infection in this survey included sourcing water from streams, which had a higher prevalence (40.0%) than those who sourced water from taps (0.0%). Frequent contact with large water bodies also showed a higher prevalence (35.8%) than those who did not have contact with water bodies (34.7%) (Table 3). The age group of 16-20 years had the highest prevalence (40.5%), while the age group of 6-10 years had the lowest prevalence (29.8%) of infection. Schistosoma haematobium infection was significantly associated with age group (χ2 = 50.6220, p = 0.0000) (Table 4).
This finding aligns with previous reports in the study area and could be attributed to the fact that older Almajirai are more actively involved in recreational and domestic activities, such as fishing, swimming, irrigation and washing their clothing in rivers, streams and dams, compared to the younger age groups2,14. Furthermore, participants who passed bloody urine had a higher prevalence (49.7%) than those who did not (17.1%) and infection with S. haematobium was significantly associated with passing bloody urine (χ2 = 58.2460, p = 0.0000). The presence of blood in the urine (hematuria) is a common symptom of urinary bilharziasis16. Similarly, those without a history of praziquantel treatment had a higher prevalence (40.2%) than those who had received praziquantel treatment (34.7%) (Table 5). These findings are consistent with previous studies that reported cultural practices and socioeconomic factors as risk factors for transmitting urinary schistosomiasis in Nigeria9,17.
This study found moderate-risk prevalence (35.6%) for urinary schistosomiasis among Almajirai and highlights significant risk factors associated with S. haematobium infection among these populations in Dutsin-Ma, Safana and Kurfi Towns. Key risk factors include drinking water sources, frequent contact with water bodies and lack of praziquantel treatment. The findings underscore the vulnerability of Almajirai, who are more likely to be reservoirs for the parasites and the importance of blood in the urine (hematuria) as a common clinical symptom. Additionally, cultural practices and socioeconomic factors play a critical role in transmitting urinary schistosomiasis. These findings emphasize the need for targeted public health interventions, including improved access to treatment and preventive measures, to control the spread of the disease in at-risk populations. Regular mass deworming programs should be scaled up for the Almajirai population in the study areas to reduce the prevalence of urinary schistosomiasis. Access to clean water should be provided and water sources should be regularly monitored for snail intermediate hosts and treated appropriately with molluscicides. Public education campaigns on the risks and transmission of urinary schistosomiasis should be launched to raise awareness among the population and encourage improved environmental sanitation and personal hygiene practices to prevent the further spread of the infection.
This study only focused on Almajirai in a few Local Government Areas in Katsina State, Nigeria, which may be subject to a recall bias. Further research should be conducted on the prevalence and risk factors of urinary schistosomiasis among the general population in the region to provide more comprehensive data that can inform better interventions for the disease.
CONCLUSION
This study identified a 35.6% prevalence of urinary schistosomiasis among the Almajirai population, classifying the study localities as moderate-risk areas (<50% prevalence). Key risk factors included frequent contact with water bodies, age and limited access to praziquantel treatment. These findings highlight the need for targeted interventions, such as mass deworming programs, improved access to clean water, enhanced environmental sanitation and public education on hygiene and disease prevention to mitigate further transmission in this vulnerable population.
SIGNIFICANCE STATEMENT
This study discovered that urinary bilharziasis remains endemic in Nigeria, providing valuable insights into its current prevalence and associated risk factors among Almajirai in thirteen schools across three Local Government Areas of Katsina State, Nigeria. The findings highlight the critical need for sustained efforts to improve environmental sanitation, ensure access to clean water and implement regular mass deworming programs for Almajirai to curb the disease’s transmission. This study will help inform disease control and prevention strategies in resource-constrained settings. Consequently, targeted intervention focusing on sustainable strategies for combating urinary bilharziasis may be developed.
ACKNOWLEDGMENTS
The authors appreciate the support of the Katsina State Ministry of Health and the authorities of Tsangaya schools in the Safana, Dutsin-Ma and Kurfi Local Government Areas for their cooperation in permitting us to conduct this survey. We also thank the participants who volunteered to take part in the survey. Additionally, the authors acknowledge the efforts of Mr. Tayo Abdulkadir from the Department of Geography and Regional Studies, Federal University Dutsin-Ma, Katsina State, Nigeria, for preparing the maps of the study localities.
REFERENCES
- Golan, R., C.M. Gower, A.M. Emery, D. Rollinson and J.P. Webster, 2008. Isolation and characterization of the first polymorphic microsatellite markers for Schistosoma haematobium and their application in multiplex reactions of larval stages. Mol. Ecol. Resour., 8: 647-649.
- Auta, T., J.J. Ezra, H.S. Rufai, E.D. Alabi and E. Anthony, 2020. Urinary schistosomiasis among vulnerable children in security challenged district of Safana, Katsina State-Nigeria. Int. J. Trop. Dis. Health, 41: 73-81.
- Toor, J., R. Alsallaq, J.E. Truscott, H.C. Turner and M. Werkman et al., 2018. Are we on our way to achieving the 2020 goals for schistosomiasis morbidity control using current World Health Organization guidelines? Clin. Infect. Dis., 66: S245-S252.
- Santos, J., J. Chaves, H. Araújo, N. Vale and J.M. Costa et al., 2015. Comparison of findings using ultrasonography and cystoscopy in urogenital schistosomiasis in a public health centre in rural Angola. S. Afr. Med. J., 105: 312-315.
- Boissier, J., S. Grech-Angelini, B.L. Webster, J.F. Allienne and T. Huyse et al., 2016. Outbreak of urogenital schistosomiasis in Corsica (France): An epidemiological case study. Lancet Infect. Dis., 16: 971-979.
- Gregory, D.M., S. Mohammed and S. Halilu, 2023. Review of Almajiri education system in Nigeria. Int. J. Educ. Natl. Dev., 1: 11-18.
- WHO, 2018. Global Status Report on Alcohol and Health 2018. World Health Organization, Switzerland, ISBN: 978-92-4-156563-9, Pages: 450.
- Bamgbola, O.F., 2014. Urinary schistosomiasis. Pediatr. Nephrol., 29: 2113-2120.
- Gamde, S.M., A. Garba, P. Tongvwam, S.D. Gamde, D.D. Agom and I. Igbinosa, 2023. Prevalence, intensity, and risk factors of urinary schistosomiasis among primary school children in Silame, Sokoto, Nigeria. Microbes Infect. Dis., 4: 695-703.
- Aribodor, O.B., N.O. Azugo, E.C. Jacob, U.C. Ngenegbo and N.D. Onwusulu et al., 2024. Assessing urogenital schistosomiasis and female genital schistosomiasis (FGS) among adolescents in Anaocha, Anambra State, Nigeria: Implications for ongoing control efforts. BMC Public Health, 24.
- Nduka, F., O.J. Nebe, N. Njepuome, D.A. Dakul and I.A. Anagbogu et al., 2019. Epidemiological mapping of schistosomiasis and soil-transmitted helminthiasis for intervention strategies in Nigeria. Niger. J. Parasitol., 40: 218-225.
- Balogun, J.B., B. Adewale, S.U. Balogun, A. Lawan and I.S. Haladu et al., 2022. Prevalence and associated risk factors of urinary schistosomiasis among primary school pupils in the Jidawa and Zobiya Communities of Jigawa State, Nigeria. Ann. Global Health, 88.
- Olamiju, F., O.J. Nebe, H. Mogaji, A. Marcus and P. Amodu-Agbi et al., 2022. Schistosomiasis outbreak during COVID-19 pandemic in Takum, Northeast Nigeria: Analysis of infection status and associated risk factors. PLoS ONE, 17.
- Atalabi, T.E., U. Lawal and S.J. Ipinlaye, 2016. Prevalence and intensity of genito-urinary schistosomiasis and associated risk factors among junior high school students in two local government areas around Zobe Dam in Katsina State, Nigeria. Parasites Vectors, 9.
- Bawa, J.A., T. Auta, I. Msughter and Y.A. Umar, 2016. Urinary schistosomiasis among primary school children in Dutsin-Ma Town, Katsina State, Nigeria. Annu. Res. Rev. Biol., 10.
- Knopp, S., S.M. Ame, J. Hattendorf, S.M. Ali and I.S. Khamis et al., 2018. Urogenital schistosomiasis elimination in Zanzibar: Accuracy of urine filtration and haematuria reagent strips for diagnosing light intensity Schistosoma haematobium infections. Parasites Vectors, 11.
- Amuta, E.U. and R.S. Houmsou, 2014. Prevalence, intensity of infection and risk factors of urinary schistosomiasis in pre-school and school aged children in Guma Local Government Area, Nigeria. Asian Pac. J. Trop. Med., 7: 34-39.
How to Cite this paper?
APA-7 Style
Rufai,
H.S., Auta,
T., Orpin,
J.B., Alabi,
E.D. (2025). Risk Factors Associated with Urinary Schistosomiasis and its Spatial Distribution Among Almajirai in Selected Localities in Katsina State, Nigeria. Asian Science Bulletin, 3(1), 63-71. https://doi.org/10.3923/asb.2025.63.71
ACS Style
Rufai,
H.S.; Auta,
T.; Orpin,
J.B.; Alabi,
E.D. Risk Factors Associated with Urinary Schistosomiasis and its Spatial Distribution Among Almajirai in Selected Localities in Katsina State, Nigeria. Asian Sci. Bul 2025, 3, 63-71. https://doi.org/10.3923/asb.2025.63.71
AMA Style
Rufai
HS, Auta
T, Orpin
JB, Alabi
ED. Risk Factors Associated with Urinary Schistosomiasis and its Spatial Distribution Among Almajirai in Selected Localities in Katsina State, Nigeria. Asian Science Bulletin. 2025; 3(1): 63-71. https://doi.org/10.3923/asb.2025.63.71
Chicago/Turabian Style
Rufai, Hafsat, Sada, Timothy Auta, James Bemshima Orpin, and Emmanuel Dayo Alabi.
2025. "Risk Factors Associated with Urinary Schistosomiasis and its Spatial Distribution Among Almajirai in Selected Localities in Katsina State, Nigeria" Asian Science Bulletin 3, no. 1: 63-71. https://doi.org/10.3923/asb.2025.63.71

This work is licensed under a Creative Commons Attribution 4.0 International License.