Understanding Buruli Ulcer in Imo State, Nigeria: Community Knowledge, Beliefs, and Treatment Compliance with WHO Guidelines
-
Onwuka, Chigozie Divine

Department of Applied and Environmental Biology, Imo State University, Owerri, PMB 2000, Nigeria
Oparaocha Evangeline TochiDepartment of Public Health, Federal University of Technology, Owerri, Nigeria
| Received 04 Jun, 2025 |
Accepted 20 Nov, 2025 |
Published 31 Dec, 2025 |
Background and Objective: Mycobacterium ulcerans is the causative agent of Buruli ulcer (BU) disease, a chronic and crippling illness that is a major public health concern in endemic areas like Nigeria. This study investigates the knowledge, attitudes, and treatment choices of people with Buruli ulcer disease in Imo State, Nigeria, as well as determining the variables affecting adherence to WHO standards. Materials and Methods: This study adopted a mixed-methods design, integrating both quantitative and qualitative approaches to comprehensively investigate the knowledge, perceptions, treatment-seeking behaviors, and adherence to World Health Organization (WHO) recommended Buruli ulcer (BU) treatment guidelines among healthcare providers and community members in Imo State, Nigeria. Healthcare providers and community members in 32 localities in Imo State, Nigeria, were surveyed (n = 360) and interviewed in-depth (n = 32). Descriptive and inferential statistical analyses (frequencies, percentages, means, standard deviations, Chi-square tests, and p-values at α = 0.05) were employed to analyze and compare the study variables. Results: Despite respondents' high degree of knowledge (93.9%) of BU illness, the study found that misconceptions regarding its etiology and transmission remained. The most common treatment-seeking behaviors were self-medication (56.7%) and herbal therapy (22.2%), and 73.3% of respondents said they followed WHO recommendations. Although 73.3% of respondents reported adherence to WHO-recommended treatment, qualitative findings revealed that such compliance was frequently inconsistent or interrupted due to cost barriers, mistrust of antibiotics, fear of amputation, and pressure from family members to seek traditional healing. Conclusion: This study emphasizes the necessity of focused initiatives to dispel myths and encourage community members and healthcare professionals in BU-endemic areas to follow WHO recommendations. Preventing deformities and enhancing disease management require improving early detection of BU disease and community health education.
INTRODUCTION
Necrotizing skin lesions are a hallmark of Buruli ulcer disease (BUD), a chronic and debilitating condition caused by Mycobacterium ulcerans1. The BUD is the third most common mycobacterial infection in humans and remains a major public health concern in 33 countries across the Western Pacific, South America, and Africa1. Each year, over 7,000 new cases are reported globally, with the majority occurring in West Africa. Despite its severity and disfiguring consequences, BUD has historically received limited attention from the global health community1.
The burden and spread of BUD are influenced by multiple interconnected factors, including entrenched superstitious beliefs, delayed disease recognition, and insufficient knowledge of the disease’s etiology2. Emerging research continues to explore the potential role of aquatic insects as vectors in the transmission of M. ulcerans3.
The BUD primarily affects rural populations living in wetland environments, where the disease’s prevalence has been closely linked to proximity to stagnant or slow-moving water bodies4. If left untreated, BUD leads to extensive skin ulceration, long-term disability, and social stigma, contributing to significant socioeconomic hardship. Its status as the third most prevalent mycobacterial infection underscores the urgency of addressing its public health implications1.
The World Health Organization has designated BUD a neglected tropical disease and emphasized the importance of early diagnosis, antibiotic treatment, and awareness campaigns to reduce disease burden1. In Nigeria, particularly in Imo State, community perceptions of BUD vary considerably and are shaped by cultural and religious beliefs5. Despite lacking biomedical validation, traditional healers and herbal remedies are frequently preferred, reflecting diverse treatment-seeking behaviors6. While the WHO recommends a combination of antibiotics and surgery for effective management, access to these services remains a significant barrier in many affected areas7.
This study aims to assess the level of community awareness, beliefs, and treatment-seeking behaviors related to BUD in Imo State, Nigeria, and to evaluate adherence to the WHO-recommended control strategies.
MATERIALS AND METHODS
Research design and methodology: This mixed-methods study examined the challenges of managing Buruli ulcer illness in endemic locations using a cross-sectional survey methodology over 24 months (September, 2022-August, 2024). The study combined quantitative and qualitative research techniques to give a thorough grasp of the issue under investigation.
Study setting: Imo State, in the Southeast Region of Nigeria, was chosen as the study area. The estimated population of Imo State is 5,459,300 (NPC, 2022), making up 3.8% of Nigeria’s total population. Covering 5,100 square kilometers, the state is located between 4°45' and 7°15' North latitude and 6°50' and 7°25' East longitude as well.
Geographically, Imo State is bordered to the North by Anambra State, to the East by Abia State, and to the South and West by Rivers State. Owerri, Okigwe, and Orlu are the three senatorial zones that make up the state, which also has 27 Local Government Areas (LGAs). The state’s three largest urbanized cities are Owerri, Okigwe, and Orlu, although the remainder of the population is spread among numerous rural areas.
The state’s economy is varied, with the main industries being small-scale manufacturing, tourism, sand mining, stone quarrying, fishing, trading, crop and animal farming, and government service. Numerous public and private schools, as well as a number of universities and colleges, make up the state’s well-established educational system.
Imo State boasts 1,338 medical facilities dispersed among 27 LGAs. The Federal Medical Center, a public tertiary hospital in the state, acts as a referral hub for all other lower-level medical facilities. The public hospital provides additional medical services through several private hospitals, such as the German Leprosy and Tuberculosis Relief Association (GLRA).
Out of the 27 LGAs in Imo State, 32 localities were chosen at random for this study. These settlements are situated in regions where Buruli ulcer disease is endemic and at high risk.
Study population: Purposively, the study population was chosen to include a wide variety of stakeholders, such as: Patients with Buruli ulcer disease: People with Buruli ulcer disease who are sourced from medical facilities and community settings
| • | Traditional healers: Medical professionals with a focus on traditional medicine who are found through community recommendations and local networks | |
| • | Healthcare professionals: Physicians hired from medical facilities that specialize in the diagnosis, management, and treatment of Buruli ulcer illness | |
| • | Elderly community members: Esteemed elders in the community who are familiar with the customs, cultural values, and background of Buruli ulcer illness | |
| • | Household heads are chosen from communities where Buruli ulcer disease is endemic and are in charge of making decisions for their households |
Sampling methodology: The study used a multistage sampling strategy that combined non-probability and probability sampling methods. With the use of Epi-Info 20 software, the estimated population of the 32 communities that were chosen came to 4,285. For the community survey, 360 respondents were considered a suitable sample size.
Sample size estimation: A total of 360 participants were selected for the quantitative survey using a multistage sampling technique. The sample size was calculated using Leslie Fischer’s formula, which is appropriate for populations larger than 10,000. The correction formula was then applied to adjust for the actual finite population size8. This ensured that the selected sample was statistically representative of the target population across Buruli ulcer-endemic communities in Imo State.
Using Leslie Fischer’s calculation, the sample size was determined for populations larger than 10,000:
Where:
| n | = | Minimum required sample size | |
| z | = | 1.96 (standard normal deviate at 95% confidence) | |
| p | = | 0.72 (estimated proportion of individuals aware of BU) | |
| q | = | 1-p = 0.28 | |
| d | = | 0.05 (desired level of precision) |
Substituting these values, we obtained:
Since the target population (N) was finite (N = 4,325), a correction was applied using the formula:
nf = 1+4325 (309.74) (309.74) ≈1.0716 (309.74) ≈289
Thus, the final sample size was rounded up to 289 to ensure representativeness and account for potential non-response.
Note: While the actual sample size used in the study was 360 (greater than the required 289), this was done intentionally to enhance statistical power and subgroup analysis, especially given the mixed-methods nature of the research.
Instrumentation for data collection: Data were gathered utilizing a mixed-method approach that included both quantitative and qualitative methods. Qualitative information was acquired by reviewing respondents medical records and documents.
| • | Conducting key informant interviews with community people and stakeholders to get comprehensive information | |
| • | Group discussions with Buruli ulcer patients and community members | |
| • | Observational studies at government clinics and traditional healing facilities |
Three hundred and sixty community members completed a semi-structured questionnaire to collect quantitative data on demographics, disease prevalence and knowledge, community attitudes and preferred treatment techniques, and adherence to the WHO-recommended management regimen.
Data collection procedures: Two research assistants were trained for two days on study questions, data gathering methodologies, and languages. The department issued a letter of introduction, which enabled the researcher and trained assistants to meet with key stakeholders. Individuals with poor literacy levels were given vernacular explanations, while the questionnaire was filled out in English.
Furthermore, six key informant interviews with medical professionals were conducted to investigate systemic issues, notably those related to Buruli ulcer control programs. The primary informants included healthcare administrators and providers, the head of the Nigerian Ministry of Health in Imo State, and health officers in charge of multiple clinics.
Participant criteria
Inclusion criteria: Participants in the study must have met the following requirements:
| • | Adults (18 and older), both men and women | |
| • | Adults with confirmed Buruli ulcer disease, as verified by polymerase chain reaction (PCR) or acid-fast bacilli staining microscopy |
The criteria for exclusion: Those who met any of the following conditions were not permitted to participate in the study.
| • | People who suffer ulcers as a result of serious traumas such as burns, home accidents, or car accidents | |
| • | People who, either directly or through a parent or legal agent, are unable to give informed consent |
Instrument validation and reliability: To enhance the validity and depth of interpretation, the study employed a triangulation method, integrating both quantitative survey data and qualitative interview findings. This methodological triangulation helped to cross-verify responses and strengthen the reliability of observed patterns, particularly in understanding community beliefs and treatment behaviors toward Buruli ulcer9. The questionnaire was tested for reliability using the Cronbach’s alpha method, which measures the internal consistency of items within the instrument. A Cronbach’s alpha value of 0.70 or higher was considered acceptable for reliability assessment10.
Ethical consideration: To protect human participants and ensure the investigation's integrity, strict ethical procedures were followed in this study. The Imo State Ministry of Health and the Ethics Review Committee of the Federal University of Technology, Owerri (FUTO) School of Public Health both gave their clearance. Each respondent provided informed consent to ensure confidentiality, anonymity, and the right to withdraw from the study at any time.
Data analysis: To address the study objectives and analyze the variables of interest, descriptive and inferential statistical analyses were conducted. Descriptive statistics included studies of frequencies, percentages, averages, and standard deviations. Inferential statistics used p-values and Chi-square tests to assess correlations between variables, while tabulations and cross-tabulations were created to provide a basic description of the variables and facilitate comparisons. The study’s significance level was set at α = 0.05.
The study employed unpaired t-tests to assess the hypothesis and evaluate the relationships between respondents' preferred treatment approaches, perceptions, and adherence to the WHO-recommended Buruli ulcer regimen in Imo State. The results were presented as graphs, bar charts, and tabular data to facilitate interpretation.
RESULTS
Respondents' socio-demographic characteristics: The study had a total of 360 respondents. Table 1 provides the respondents' socio-demographic information:
| • | Gender distribution: The gender distribution demonstrated a modest preference for females (52.5%, n = 189) over males (47.5%, n = 171) | |
| • | Age distribution: The majority of respondents (67.8%, n = 244) fell between the ages of 18 and 57, according to the age distribution | |
| • | Educational background: The respondents lacked formal schooling, with 52.2% (n = 188) being analphabets | |
| • | Distribution by occupation: According to the occupational breakdown, 22.2% (n = 80) of respondents were mostly involved in farming | |
| • | The average age among respondents was [3.2] years (±0.057) |
Buruli ulcer disease prevalence in selected endemic local government areas: The frequency of Buruli ulcer illness differed significantly across the chosen local government regions (Fig. 1). The highest prevalence was in Oguta with 72 cases (20.0%), followed by Ohaji Egbema with 60 cases (16.61%) and Mbaitolu with 46 cases (12.77%). In comparison, Ideato South had the lowest prevalence, with 16 occurrences (4.40%).
Buruli ulcer disease
Community knowledge and awareness: The findings provide useful insights into respondents’ knowledge and information sources on Buruli ulcer disease (BUD) in the study area. According to Table 2, the majority of respondents (93.9%) were aware of BUD, with 83.3% correctly identifying painless itching/burning sensations as a sign or symptom of the condition.

|
| Table 1: | Socio-demographic characteristics of community | |||
| Characteristics | Frequency (N = 360) | Percentage |
| Sex | ||
| Female | 189 | 52.5 |
| Male | 171 | 47.5 |
| Age group (years) | ||
| 18-31 | 30 | 8.3 |
| 32-44 | 104 | 28.9 |
| 45-57 | 110 | 30.6 |
| 58-Above | 116 | 32.2 |
| Educational qualification | ||
| No formal education | 188 | 52.2 |
| Primary | 92 | 25.6 |
| Junior high school | 39 | 10.8 |
| Senior high school | 24 | 6.7 |
| Vocational/technical | 7 | 1.9 |
| Tertiary | 10 | 2.7 |
| Occupational status | ||
| Unemployed | 15 | 4.2 |
| Civil servant | 9 | 2.5 |
| Trading | 80 | 22.2 |
| Farming | 184 | 51.1 |
| Laborers/sand quarry | 38 | 10.6 |
| Fishing | 22 | 6.1 |
| Others (mining, cobblers) | 12 | 3.3 |
| Total | 360 | 100% |
Respondents’ top information sources were community volunteers (58.9%), patients (17.1%), and health centers (7.2%). This underscores the importance of community-based initiatives and human communication in disseminating information about BUD. The limited reliance on media (5.8%) and rumor (3.8%) as information sources shows that tailored health education and community engagement efforts may be more effective in raising awareness and comprehension of BUD.
|
| Table 2: | Distribution of knowledge and source of information in BUD by respondents | |||
| Characteristics | Frequency (N = 360) | Percentage |
| (Blisters, plague and nodules) | ||
| Yes | 338 | 93.9 |
| No | 22 | 6.1 |
| Sources of information | ||
| Community volunteers | 212 | 58.9 |
| Patients | 62 | 17.1 |
| Media | 21 | 5.8 |
| Health centre | 26 | 7.2 |
| Former Buruli ulcer patients | 25 | 7.2 |
| Rumor | 14 | 3.8 |
| Signs and symptoms | ||
| Painless, itchy/burning sensation | 300 | 83.3 |
| Sour | 60 | 16.7 |
| Causes | ||
| Natural | 172 | 47.8 |
| Supernatural | 182 | 50.5 |
| Natural and supernatural | 6 | 1.6 |
| Total | 360 | 100 |
Qualitative perspectives: Respondents were also questioned about the sources of their awareness, with the findings shown in Table 2. A critical source shared their understanding of Buruli ulcer illness, describing it as:
"Buruli ulcer, a devastating skin disease caused by the bacterium Mycobacterium ulcerans, usually starts with a painless swelling known as a nodule. However, it can also present as a painless plaque on the leg or face, referred to as oedema, and is commonly characterized by the presence of necrotic, cotton wool-like tissues at its boundaries”.
Surprisingly, respondents’ beliefs of the causes of BUD were evenly divided between natural (47.8%) and supernatural (50.5%) explanations, with a small fraction (1.6%) attributing the condition to both natural and supernatural sources. This ambivalence emphasizes the importance of culturally responsive health education and awareness-raising activities that address the complicated interplay between traditional beliefs and modern healthcare practice.
| Table 3: | Community perceptions and beliefs about Buruli ulcer diseases | |||
| Characteristics | Frequency (N = 360) | Percentage |
| Bewitched | 150 | 41.7 |
| Lack of hygiene | 84 | 3.3 |
| Sustained wounds | 51 | 14.2 |
| Insects bites | 40 | 11.1 |
| Normal sick people | 35 | 9.7 |
| Transmission | ||
| Contagious | 233 | 64.7 |
| Non-contagious | 116 | 32.2 |
| No Idea | 113.1 | |
| Treatment | ||
| It can be cured | 316 | 87.8 |
| It cannot be cured | 44 | 12.2 |
| Preferred mode of treatment | ||
| Orthodox medicine | 119 | 33.1 |
| Conventional healers | 188 | 52.2 |
| Orthodox and secular | 53 | 14.7 |
| Total | 360 | 100% |
| Table 4: | Respondents’ preferred treatment methods for BUD | |||
| Variables | Frequency | Percentage |
| Treatments | ||
| Immediate | 290 | 80.1 |
| Wait | 70 | 19.9 |
| Place of treatment | ||
| Traditional healer | 80 | 22.2 |
| Pharmacy/drug store | 204 | 56.7 |
| Prayer house | 18 | 5 |
| Health facilities | 50 | 13.9 |
| Did nothing | 8 | 2.2 |
| Distribution of health facilities available | ||
| Health facilities | ||
| Drug store | 253 | 70.3 |
| Hospitals/Clinics | 40 | 11.1 |
| Herbal treatment | 47 | 13.1 |
| Prayer House | 16 | 4.4 |
| Distribution of health facilities frequently used | ||
| Pharmacy/drugstore | 204 | 56.7 |
| Clinic/hospital | 46 | 12.8 |
| Traditional healer | 88 | 24.4 |
| Prayer house | 22 | 6.1 |
| Distance to the health facilities | ||
| Close | 268 | 74.4 |
| Far | 92 | 25.6 |
| System of transportation to health facilities | ||
| Oka (da/Tricycle | 100 | 27.8 |
| Car (Taxi and private) | 42 | 11.7 |
| Bicycle | 14 | 3.9 |
| Walk | 204 | 56.6 |
| Total | 360 | 100% |
Community perceptions and beliefs about buruli ulcer diseases: Table 3 shows community attitudes of Buruli ulcer patients in Imo State, Nigeria. The findings show a complicated interplay between traditional beliefs, misconceptions, and disease knowledge.
Notably, a large majority of respondents (41.7%) believed that Buruli ulcer patients were cursed, demonstrating the persistent influence of traditional beliefs on disease perception.
In terms of transmission, the majority of respondents (64.7%) said Buruli ulcer is contagious, while 32.2% believed it is not. This discrepancy highlights the importance of focused health education in clarifying the mode of transmission and preventing additional stigmatization of affected persons.
Fortunately, the majority of respondents (87.8%) believed that Buruli ulcers could be treated, which is critical for good disease treatment and control. However, the chosen style of treatment demonstrated a considerable dependence on conventional healers (52.2%), with 33.1% choosing orthodox medicine and 14.7% choosing a combination of the two. This emphasizes the importance of integrated healthcare techniques that embrace both traditional and modern practices.
Qualitative insights: In-depth interviews offered further information about community perspectives and reactions. One respondent noted the difficulties of socializing with Buruli ulcer patients because of the terrible odor from their wounds. Another respondent provided a personal story, claiming that they caught the ailment while visiting a friend with a Buruli ulcer.
Respondents’ preferred buruli ulcer treatment methods: Table 4 shows the recommended treatment strategies for Buruli ulcer disease (BUD) among respondents in the study area. The findings illustrate the intricate relationship between traditional and modern healthcare methods.
Notably, the vast majority of responders (80.1%) recommended immediate treatment for BUD, while 19.9% chose to wait. This finding implies that responders understand the significance of quick treatment for BUD. However, the chosen place of treatment revealed a considerable reliance on traditional healers (22.2%) and pharmacy/drug stores (56.7%), with a lesser number choosing health facilities (13.9%). This emphasizes the importance of integrated healthcare techniques that embrace both traditional and modern practices.
Focus group sessions with key informants highlighted the difficulties of accessing healthcare facilities, such as transportation fees and delays in healthcare systems.
The distribution of health facilities available to respondents showed that pharmacy/drug stores (70.3%) and herbal treatment centers (13.1%) were the most common options. However, the distribution of health facilities frequented by respondents suggested a considerable reliance on pharmacy/drug stores (56.7%) and traditional healers (24.4%). This implies that respondents prefer convenient and accessible healthcare options, even if they might not always deliver the best care.
Focus groups with key informants highlighted the problems of accessing healthcare facilities, including transportation fees and delays.
The majority of respondents (74.4%) claimed that health facilities were close to their homes, while 25.6% said they were far away. This finding shows that geographic availability to healthcare institutions may not be a substantial barrier to BUD treatment in this population. However, the transportation system to health institutions demonstrated a considerable reliance on walking (56.6%) and okadas/tricycles (27.8%), with a lesser proportion utilizing cars/taxis (11.7%) and bicycles (3.9%). This emphasizes the need for economical and accessible transportation options for facilitating access to healthcare institutions.
According to the survey, 80.1% of respondents would seek treatment right away if they noticed signs and symptoms of a Buruli ulcer, while 19.9% would wait to see whether their health deteriorated before seeking help. Respondents' preferred treatment techniques varied, with 22.2% choosing herbalists and 56.7% opting for self-medication (Table 4).
| Table 5: | The relationship between sex, age, education, and the first line of treatment for buruli ulcers | |||
| The first line of treatment |
Female N = 189 (%) |
Male N = 171 (%) |
p-value | Chi-square | Degree of freedom |
| Self-medication | 80 (42.32) | 63(36.84) | 0.781097 | 5.6 | |
| Health centre | 59 (31.21) | 58 (33.91) | 0.778733 | 7.23 | 3 |
| Traditional treatment | 47 (24.86) | 42 (24.56) | 0.99 | 23 | |
| Prayer house | 3 (1.75) | 8(4.68) | 0.001 | ||
| Age group | 18-43 yrs | 44 yrs and above | |||
| N =134 (%) | N = 226 (%) | ||||
| Self-medication | 58 (43.28) | 100 (44.25) | 0.001667 | 16.67 | |
| Health centre | 30 (22.38) | 62 (27.43) | 0.008961 | 20.91 | 3 |
| Traditional treatment | 40 (29.85) | 57 (25.22) | 0.060231 | 15.12 | |
| Prayer house | 8 (5.97) | 7 (3.10) | 0.15 | ||
| Education | No education | Primary and above | |||
| N = 188 (%) | N = 172 (%) | ||||
| Self-medication | 93 (49.47) | 48( 27.91) | 0.0012 | 31.23 | |
| Health centre | 46 (24.47) | 74 (43.02) | 0.00976 | 22.54 | 3 |
| Traditional treatment | 45 (23.94) | 44 (25.58) | 0.31817 | 7.76 | |
| Prayer house | 4 (2.13) | 6 (3.49) | - | - |
| Table 6: | Relationship between gender, age, education, and participants who favored immediate treatment for Buruli ulcer | |||
| Preferred treatment Immediately |
Female N = 189 (%) |
Male N = 171 (%) |
p-value | Chi square value |
Degree of Freedom |
| Yes | 140 (74.1) | 120 (70.17) | 0.888045 | 9.28 | |
| No | 44 (23.28) | 48 (28.07) | 0.968701 | 9.87 | 2 |
| Did nothing | 5 (2.64) | 3 (1.75) | 0.43 | ||
| Age | 18-43 years | 44 and Above | |||
| N = 134 (%) | N = 226 (%) | ||||
| Yes | 90 (67.16) | 170 (75.22) | 0.001 | 33.41 | |
| No | 44 (32.83) | 56 (24.77) | 0.048157 | 15.57 | 2 |
| Educational | |||||
| Status | No education | Primary and above | |||
| N = 194 (%) | N = 166 (%) | ||||
| Yes | 140 (72.16) | 116 (69.87) | 0.033602 | 15.43 | |
| No | 54 (27.83) | 50 (30.12) | 0.190234 | 0.21 | 2 |
Table 5 depicts the link between socio-demographic characteristics and the first line of treatment for Buruli ulcer in the study area.
Sex and treatment-seeking behavior: There was no statistically significant difference in treatment-seeking behavior between males and females (p>0.05). However, a slightly higher proportion of females (42.32%) reported self-medication as their initial treatment compared to males (36.84%).
Age and treatment-seeking behavior: A significant difference was observed in treatment-seeking behavior across age groups (p<0.01). Younger individuals (18-43 years) were more likely to engage in self-medication (43.28%) and traditional treatment (29.85%) as their first line of care, compared to older individuals (44 years and above).
Education and treatment-seeking behavior: Treatment-seeking behavior also varied significantly with educational level (p<0.01). Individuals with no formal education reported higher rates of self-medication (49.47%) and traditional treatment (23.94%) as their initial approach, in contrast to those with primary education or higher.
Therefore, the findings indicate that females, younger individuals, and those with lower levels of education are more inclined to use self-medication or traditional treatment as their first response to illness.
Table 6 shows the association between socio-demographic characteristics and preferences for rapid Buruli ulcer treatment.
Preferences for sex and treatment: Males and females show no significant difference in their preference for immediate treatment (p = 0.888). However, significantly more ladies (74.1%) than males (70.17%) stated a desire for immediate treatment. This shows that females are more likely to seek immediate medical assistance for a Buruli ulcer, while further study is needed to corroborate this finding.
Age and treatment preferences: The findings indicate that there is a substantial difference in the preference for quick treatment across age groups (p = 0.001). A greater proportion of elderly people (75.22%) than younger people (67.16%) indicated wanting quick care. This shows that older people are more likely to realize the necessity of seeking immediate medical assistance for a Buruli ulcer, while further study is needed to validate this conclusion.
Educational and treatment preferences: The data show that there is a considerable variation in the preference for immediate treatment amongst those with different levels of education. Individuals with primary education or higher (69.87%) preferred immediate treatment more than those with no education (72.16%). However, the difference was not statistically significant, indicating that education level may not be a powerful predictor of treatment choices.
This finding suggests that older people may be more likely to realize the significance of seeking quick medical assistance for a Buruli ulcer, though more research is needed to confirm this. These findings have significant implications for developing successful public health interventions and education campaigns targeted at promoting quick treatment seeking for Buruli ulcer.
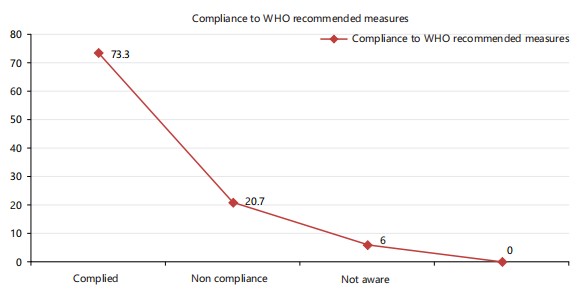
Compliance with the WHO recommended control regime for buruli ulcer: Adherence to the World Health Organization’s (WHO) recommended control regime is critical for efficient Buruli ulcer therapy. This study looked into respondents' adherence to the prescribed WHO Buruli ulcer management protocol and how they integrated it into their daily lives.
The findings show that 73.3% of respondents followed the prescribed control regime, whereas 20.7% did not. These findings highlight the necessity of adherence to comprehensive health education, early detection of occurrences, community-based surveillance, capacity building, health facility strengthening, and collaboration among stakeholders in the research region to monitor Buruli ulcer.
The use of WHO-recommended antimicrobials (rifampicin and streptomycin) by health officers, particularly for early lesions, has been successful. Compliance with these tactics was supported by substantial coordination and coverage across the respondents' entire community. Community-based surveillance volunteers were critical in tracking, case identification, and referral, functioning as major stakeholders in society and health clinics.
These findings underline the importance of ongoing efforts to encourage compliance with the WHO-recommended control regime, including increased community-based surveillance, capacity building, and stakeholder collaboration. This can help improve early detection, treatment results, and overall management of Buruli ulcer disease.
DISCUSSION
This study examined beliefs, treatment preferences, and adherence to WHO-recommended Buruli ulcer (BU) treatment protocols among community members in Imo State, Nigeria. The findings revealed that while community awareness of BU symptoms, particularly early signs like painless swelling or boils, was relatively high, persistent misconceptions and traditional beliefs continued to shape treatment-seeking behavior. Oguta LGA reported the highest prevalence of BU, and many respondents described first resorting to traditional treatments or home remedies before seeking biomedical care, often resulting in advanced disease stages. The perception that BU is caused by both natural and supernatural forces, including witchcraft, strongly influenced health choices. Formal education was associated with more accurate knowledge, but myths persisted across educational levels.
Respondents noted that while WHO-led interventions and health worker initiatives had improved disease awareness and access to treatment, barriers such as poor trust in antibiotics, fear of amputation, and preference for traditional healers continued to impede timely medical consultation. Many patients returned to health facilities with worsened ulcers after unsuccessful herbal treatments. Factors such as ease of access, low cost, and the cultural familiarity of traditional healers made them preferred options over formal healthcare. Nevertheless, community health workers and WHO-supported programs have facilitated progress through awareness campaigns, early case identification, and improved follow-up mechanisms.
These findings confirm previous studies conducted in similar contexts. Prior research has shown that while communities can identify early symptoms, delays in seeking biomedical care are common due to cultural beliefs and structural barriers10-13. The persistence of dual causal explanations (natural and supernatural) has also been reported14, and continued reliance on traditional medicine even when biomedical alternatives are known has been similarly documented. However, this study adds nuance by showing that even educated individuals may hold dual explanatory models, suggesting that information alone is insufficient to shift behavior without trust and engagement.
This study had several limitations. It relied heavily on qualitative self-reports, which may be subject to recall bias or socially desirable responses. The sample was geographically limited to Imo State, which may reduce the generalizability of the findings. Additionally, the study did not include quantitative outcome measures for treatment effectiveness or rates of adherence to biomedical care. Future research should incorporate longitudinal tracking of patient outcomes and evaluate the impact of integrated interventions that engage both biomedical and traditional care systems.
Based on the findings, several recommendations are proposed in alignment with the World Health Organization’s approach to Buruli ulcer (BU) control, particularly in under-resourced rural health systems. Community health education should be strengthened by emphasizing not only the recognition of symptoms but also the importance of early biomedical treatment, the risks associated with delayed care, and the correction of widespread misconceptions, such as the belief that antibiotics lead to amputation. Traditional healers and community leaders should be actively engaged in BU control strategies, as their involvement in health education and referral systems can build trust and enhance compliance with biomedical interventions. Access to diagnosis and treatment must be improved through the development of health infrastructure, the deployment of mobile health services, and the provision of transport assistance, especially in remote or high-burden local government areas like Oguta. Efforts should also focus on promoting early detection and care-seeking behaviors by encouraging individuals to promptly report boils, abrasions, and skin changes. This can be achieved through culturally relevant communication channels, including local radio, religious institutions, and schools. School-based and youth education programs are vital for fostering accurate health knowledge and dispelling stigmatizing or supernatural beliefs associated with BU. Additionally, laboratory confirmation of suspected pre-ulcerative lesions should be made mandatory to ensure diagnostic accuracy and timely intervention. Finally, surveillance and follow-up systems should be strengthened through community health volunteers, digital monitoring tools, and continuous tracking, thereby supporting early case identification, enhancing treatment adherence, and minimizing default rates.
CONCLUSION
The study highlights that while awareness of Buruli ulcer (BU) is relatively high among respondents in Imo State, deep-rooted misconceptions and socio-cultural factors continue to influence treatment choices and adherence to WHO-recommended guidelines. The widespread reliance on self-medication and herbal remedies reflects persistent gaps in trust toward biomedical interventions. Financial constraints, fear of amputation, and familial pressure to pursue traditional healing further undermine consistent compliance with treatment. Strengthening community health education, improving access to affordable medical care, and engaging traditional and community leaders are essential to bridge these gaps. Sustained public health efforts aimed at early detection, myth dispelling, and fostering collaboration between healthcare providers and the community will be critical for reducing BU-related deformities and enhancing disease management outcomes.
SIGNIFICANCE STATEMENT
Buruli ulcer is a treatable disease, but in many Nigerian communities, treatment is often delayed due to cultural beliefs and reliance on traditional medicine. This study explored how people in Imo State understand the disease and make choices about care. Despite high awareness, many still believe the disease has spiritual causes, leading them to avoid or delay biomedical treatment. These findings highlight the urgent need for culturally sensitive health education and stronger integration between traditional and modern healthcare systems. By addressing both beliefs and access, future programs can improve early treatment and prevent serious complications from Buruli ulcer.
ACKNOWLEDGMENT
My sincere gratitude goes to the study participants, community leaders, and healthcare workers in Imo State, Nigeria, for their invaluable contributions to this research. We also acknowledge the support and guidance provided by the World Health Organization's (WHO) Buruli Ulcer Control Program. This study was made possible through the collaborative efforts of the Ministry of Health, Imo State and the German Leprosy and Tuberculosis Relief Association (GLRA). We appreciate the technical assistance and resources provided by Dr Okeke Joel.
REFERENCES
- van der Werf, T.S., Y.T. Barogui, P.J. Converse, R.O. Phillips and Y. Stienstra, 2020. Pharmacologic management of Mycobacterium ulcerans infection. Expert Rev. Clin. Pharmacol., 13: 391-401.
- Yotsu, R.R., K. Suzuki, R.E. Simmonds, R. Bedimo and A. Ablordey et al., 2018. Buruli ulcer: A review of the current knowledge. Curr. Trop. Med. Rep., 5: 247-256.
- Merritt, R.W., E.D. Walker, P.L.C. Small, J.R. Wallace and P.D.R. Johnson et al., 2010. Ecology and transmission of Buruli ulcer disease: A systematic review. PLoS Negl. Trop. Dis., 4.
- Walsh, D.S., F. Portaels and W.M. Meyers, 2011. Buruli ulcer: Advances in understanding Mycobacterium ulcerans infection. Dermatologic Clin., 29: 1-8.
- Adeneye, A.K., O.P. Akinwale, S.M.C. Ezeugwu, Y.A. Olukosi and B. Adewale et al., 2024. Knowledge and perception of Buruli ulcer in communities of two endemic local government areas of Ogun State, Nigeria. Ann. Public Health Epidemiol., 2.
- Grietens, K.P., A.U. Boock, H. Peeters, S. Hausmann-Muela, E. Toomer and J.M. Ribera, 2008. “It is me who endures but my family that suffers”: Social isolation as a consequence of the household cost burden of Buruli ulcer free of charge hospital treatment. PLoS Negl. Trop. Dis., 2.
- Fisher, A.A., J.E. Laing, J.E. Stoeckel and J. Townsend, 1991. Handbook for Family Planning Operations Research Design. 2nd Edn., Population Council, New York, Pages: 77.
- Denzin, N.K., 1978. The Research Act: A Theoretical Introduction to Sociological Methods. 2nd Edn., McGraw-Hill, New York, ISBN: 9780070163614, Pages: 370.
- Tavakol, M. and R. Dennick, 2011. Making sense of Cronbach's alpha. Intl. J. Med. Educ., 2: 53-55.
- Amofah, G., F. Bonsu, C. Tetteh, J. Okrah, K. Asamoa, K. Asiedu and J. Addy, 2002. Buruli ulcer in Ghana: Results of a national case search. Emerg. Infect. Dis., 8: 167-170.
- Nienhuis, W.A., Y. Stienstra, W.A. Thompson, P.C. Awuah and K.M. Abass et al., 2010. Antimicrobial treatment for early, limited Mycobacterium ulcerans infection: A randomised controlled trial. Lancet, 375: 664-672.
- Portaels, F., M.T. Silva and W.M. Meyers, 2009. Buruli ulcer. Clin. Dermatol., 27: 291-305.
- Stienstra, Y., W.F. van der Graaf, K. Asamoa and T.S. van der Werf, 2002. Beliefs and attitudes toward Buruli ulcer in Ghana. Am. J. Trop. Med. Hyg., 67: 207-213.
- Hotez, P.J., 2023. A constitutional amendment for deworming. PLoS Negl. Trop. Dis., 3.
How to Cite this paper?
APA-7 Style
Divine,
O.C., Tochi,
O.E. (2025). Understanding Buruli Ulcer in Imo State, Nigeria: Community Knowledge, Beliefs, and Treatment Compliance with WHO Guidelines. Asian Science Bulletin, 3(4), 274-287. https://doi.org/10.3923/asb.2025.274.287
ACS Style
Divine,
O.C.; Tochi,
O.E. Understanding Buruli Ulcer in Imo State, Nigeria: Community Knowledge, Beliefs, and Treatment Compliance with WHO Guidelines. Asian Sci. Bul 2025, 3, 274-287. https://doi.org/10.3923/asb.2025.274.287
AMA Style
Divine
OC, Tochi
OE. Understanding Buruli Ulcer in Imo State, Nigeria: Community Knowledge, Beliefs, and Treatment Compliance with WHO Guidelines. Asian Science Bulletin. 2025; 3(4): 274-287. https://doi.org/10.3923/asb.2025.274.287
Chicago/Turabian Style
Divine, Onwuka,, Chigozie, and Oparaocha Evangeline Tochi.
2025. "Understanding Buruli Ulcer in Imo State, Nigeria: Community Knowledge, Beliefs, and Treatment Compliance with WHO Guidelines" Asian Science Bulletin 3, no. 4: 274-287. https://doi.org/10.3923/asb.2025.274.287

This work is licensed under a Creative Commons Attribution 4.0 International License.