Effects of Physical Activity on Depression Among Adults: A Case-Control Study
-
Waseela Ashraf

University of Europe for Applied Sciences, Dubai, United Arab Emirates
Syeda Amina BatoolUniversity Institute of Public Health, The University of Lahore, 92.45839, Punjab, Pakistan
| Received 14 Feb, 2026 |
Accepted 15 May, 2026 |
Published 30 Jun, 2026 |
Background and Objective: Depression affects millions globally, with physical activity proposed as a protective factor. This study aimed to investigate the relationship between physical activity levels and depression among adults in Poonch, AJK, Pakistan, while identifying associated socio-demographic factors. Materials and Methods: A case-control study was conducted with 112 adults (56 with depression, 56 controls) at a central military hospital, using purposive sampling. Data were collected through the Patient Health Questionnaire (PHQ-9), Global Physical Activity Questionnaire (GPAQ), and socio-demographic forms. Data were analyzed using R software 4.0.4 (RStudio 1.4.1106), with descriptive statistics, Chi-square tests for categorical variables, t-tests for continuous variables, and significance set at p≤0.05. Results: Cases exhibited significantly higher depression symptoms (p<0.0001) and lower physical activity levels (mean METs/week: 781.28 vs 1048.64, p = 0.002) compared to controls. Urban residence was associated with increased odds of depression (AOR = 2.66; 95% CI: 1.03-8.78), while higher physical activity was protective (AOR = 0.998; 95% CI: 0.997-0.999). Age, gender, marital status, education, income, job type, working hours, and BMI showed no significant associations with depression. Conclusion: Urban residence emerged as a significant independent risk factor for depression (AOR = 2.66), while higher physical activity levels demonstrated a protective effect (AOR = 0.998). These findings highlight the importance of socio-demographic context and lifestyle factors in depression etiology, suggesting that targeted interventions promoting physical activity and addressing urban-specific stressors may be particularly valuable for depression prevention in this population.
INTRODUCTION
Depression is a leading global mental health disorder, affecting approximately 5% of adults and contributing to over 700,000 suicides annually, with higher prevalence among women and older adults1. The substantial burden of depression on individuals and healthcare systems underscores the urgent need for accessible, preventive strategies. Physical activity (PA) has emerged as a robust protective factor against depression, operating through multiple biological and psychosocial pathways, including enhanced neurogenesis, regulation of the hypothalamic-pituitary-adrenal axis, reduced inflammation, improved self-esteem, and increased social support2,3. Meta-analyses and large-scale cohort studies confirm that higher levels of PA are associated with an 18-25% reduction in depression risk, with benefits observed across age groups, genders, and global regions4,5. Even moderate increases in PA, such as regular walking or aerobic exercise, confer significant mental health benefits, and acute bouts of activity can improve affective states in people with depression6,7.
Despite these well-established benefits, global PA levels remain inadequate, with only 73% of adults meeting WHO guidelines and marked disparities by gender, socioeconomic status, and geography. These gaps are particularly pronounced in conflict-affected and low-resource settings, where the mental health impact of trauma and chronic stress is compounded by limited access to care8. Systematic reviews highlight that PA not only reduces depression and anxiety after traumatic events including war, disaster, and pandemic but also promotes resilience, sleep quality, and overall well-being8. However, most evidence originates from high-income countries, and little is known about the PA-depression relationship in South Asia, especially in regions like Kashmir, where conflict-related stressors and cultural factors may uniquely shape both PA patterns and mental health outcomes.
Methodological limitations further constrain current knowledge, including reliance on self-reported PA, inadequate adjustment for confounders, and a lack of longitudinal data in young adults a critical period for depression onset9. Moreover, depression-specific barriers to PA, such as amotivation and fatigue, are poorly characterized in low- and middle-income countries, where treatment access is severely limited.
This study addresses these critical gaps by investigating the association between physical activity and depression among adults in Poonch, Azad Jammu and Kashmir (AJK), Pakistan, a region with unique sociocultural and environmental stressors. Using validated tools (PHQ-9 and GPAQ) and adjusting for key sociodemographic confounders, this research provides the first evidence on PA-depression dynamics in Kashmiri adults. The findings aim to inform low-cost, scalable interventions and contribute to Pakistan’s emerging mental health strategy, particularly as the COVID-19 pandemic has exacerbated both physical inactivity and depression in the region3,8. By bridging universal biological mechanisms with local context, this study offers actionable insights for populations facing the dual burdens of conflict and rising depression, where PA represents an accessible, sustainable prevention strategy.
MATERIALS AND METHODS
Study design: An unmatched case-control study was employed to identify factors associated with depression in relation to physical activity levels. This design was selected to efficiently examine the relationship between physical activity and depression by comparing individuals with depression (cases) to those without (controls) within the same population.
Setting: The research was conducted at the Central Military Hospital in Poonch, Azad Jammu and Kashmir (AJK), a 250-bed healthcare facility serving the local population. This setting provided access to both psychiatric services for case identification and general healthcare services for control recruitment within a controlled clinical environment.
Study duration: Data collection was carried out over six months from February 1, 2024, to July 31, 2024. This timeframe allowed for adequate participant recruitment while ensuring consistent data collection conditions throughout the study.
Sample size: The total sample comprised 112 participants, with an equal distribution of 56 cases and 56 controls. The sample size was calculated using the Fleiss method for unmatched case-control studies through Open Epi Version 3. This calculation was based on a global depression prevalence of 5%, physical activity prevalence in Pakistan of 66.5% (as reported by WHO), and a hypothetical physical activity prevalence of 40% among depressed individuals due to the absence of local data.
Sampling technique: A non-probability purposive sampling approach was utilized to select participants who met specific eligibility criteria. Cases were identified through psychiatric clinics and consultations at the hospital, where they underwent initial screening using the Patient Health Questionnaire (PHQ-9). Individuals with depressive symptoms subsequently received a comprehensive psychiatric evaluation by a certified psychiatrist to confirm a depression diagnosis based on DSM-5 criteria. Controls were selected from the same community and healthcare settings to ensure comparable environmental and demographic contexts. They were similarly screened using the PHQ-9 to confirm the absence of depressive symptoms, with a psychiatrist verifying no undiagnosed depression or other psychiatric disorders.
Sample selection: Participants were required to be adults aged 18-40 years of both genders. Exclusion criteria included individuals with Major Depressive Disorder diagnosed more than 30 days prior, those with severe medical conditions limiting physical activity (e.g., cardiovascular diseases, cancer, orthopedic issues), individuals with psychiatric conditions other than depression (such as post-traumatic stress disorder, bipolar disorder, generalized anxiety disorder, adjustment disorder, or eating disorders), and those not engaging in regular physical activity.
Study groups: Cases were defined as individuals clinically diagnosed with Major Depressive Disorder (MDD) within the last 30 days according to DSM-5 criteria. Controls were individuals without a clinical diagnosis of MDD, confirmed through psychiatric evaluation and PHQ-9 screening.
Ethical considerations: The study received ethical approval from the Research Ethics Committee (REC) at the University of Lahore, Pakistan (Reference Number: REC-UOL-/553/08/24, dated 07-05-2024), and was conducted in accordance with the committee’s established ethical guidelines. Written informed consent was obtained from all participants after ensuring they fully understood the study’s purpose, procedures, and their rights, including the right to withdraw at any time without disadvantages. Participants were informed that the study posed no significant risks, and all data collection procedures were designed to minimize discomfort. Confidentiality was maintained through participant anonymity and secure data storage, which was kept under lock and key with password protection on electronic devices. Data will be securely destroyed after the required retention period, in compliance with data protection regulations and researchers will disclose any potential conflicts of interest.
Data collection procedure: Physical activity levels were assessed using the Global Physical Activity Questionnaire (GPAQ) Version 2, which calculates weekly MET-minutes by combining moderate-intensity activity (minutes×4 MET) and vigorous-intensity activity (minutes×8 MET). Participants were classified into four categories: Physically inactive (<400 MET-minutes/week), mildly physically active (400-599 MET-minutes/week), moderately physically active (600-799 MET-minutes/week), and highly physically active (≥800 MET-minutes/week). Show cards were used to illustrate activity types and assist respondents during questionnaire administration. Participants completed the GPAQ based on their typical weekly routine before MDD diagnosis. Depression was diagnosed according to DSM-5 Criteria for Major Depressive Disorder, requiring at least five symptoms present during two weeks, including either depressed mood or loss of interest/pleasure, along with additional criteria regarding symptom severity, functional impairment, and exclusion of other medical or psychiatric conditions. The GPAQ is a validated tool for estimating physical activity levels10, while the PHQ-9 and DSM-5 criteria provide reliable methods for depression assessment with established validity and reliability. The data collection process involved participant recruitment through orientation sessions, eligibility screening, physical activity assessment via GPAQ, depression confirmation through psychiatric evaluation, and secure data recording with coding to maintain confidentiality.
|
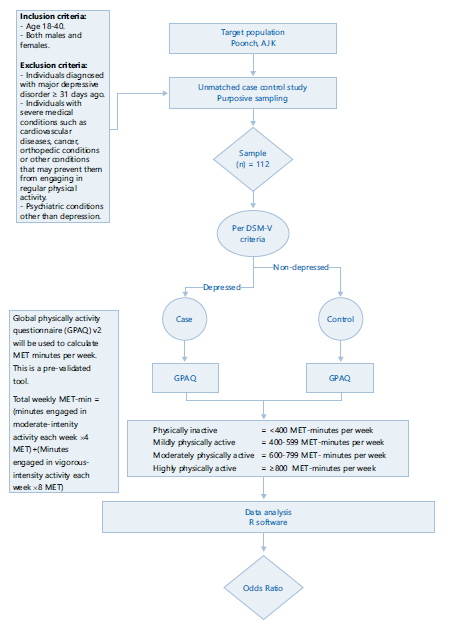
The conceptual framework and methodological flow of the study are summarized in Fig. 1. Figure 1 illustrates the systematic progression from participant recruitment to statistical inference. The target population comprised residents of Poonch, AJK (n = 112), selected via purposive sampling. Depression status (Case/Control) was the dependent variable, determined according to DSM-5 criteria, while physical activity (MET-minutes/week) served as the independent variable, measured using GPAQ v2. The framework investigates how varying physical activity levels (<400 to ≥800 MET-minutes/week) correlate with the presence of depression. Data were analyzed using R software, with odds ratios (OR) computed to quantify the influence of physical inactivity on depressive status.
Variables: The dependent variable was Major Depressive Disorder (MDD). Independent variables included physical activity level, age, gender, education, occupation, working hours, and socioeconomic status.
Data analysis procedure: Data were entered and analyzed using R software version 4.0.4 with the RStudio interface (version 1.4.1106). Descriptive statistics were computed for all variables. Frequency and percentages were calculated for categorical variables (e.g., gender, socioeconomic status, and education), whereas mean and standard deviation (±SD) were reported for continuous variables such as age, working hours, and GPAQ (Global Physical Activity Questionnaire) scores.
Group differences between cases and controls were assessed using the Chi-square test for categorical variables and the independent samples t-test for continuous variables. A p-≤0.05 was considered statistically significant.
Variables showing a significant association (p≤0.05) in the bivariate analysis were included in the multivariable logistic regression model to identify independent predictors of depression. The regression model was fitted using the generalized linear model (glm) function with a binomial family (logit link). Adjusted odds ratios (AOR) with 95% confidence intervals (CI) were computed using the exp function.
To evaluate multicollinearity among predictors, the Variance Inflation Factor (VIF) was calculated, and all variables demonstrated acceptable levels (VIF<2.0). The refined model, including residence and GPAQ score as predictors, showed improvement over the initial model (AIC reduced from 148.11 to 146.26).
RESULTS
Socio-demographic and life style factors: The study included 112 adults (56 cases and 56 controls) with a mean age of 26.72±5.36 years. The majority of participants (77.7%) were aged ≤30 years, with a nearly equal gender distribution (49.1% male, 50.9% female). Over half (56.3%) were married, and education levels varied, with 45.5% holding diplomas and 8.9% having postgraduate degrees. Employment was predominantly in the private sector (50.0%), with a mean monthly income of 37,974.11±10,913.14 PKR. Socioeconomic status was primarily middle class (58.9%), and residence was mainly urban (50.9%). Working hours were ≤8 hours for 57.1% of participants. BMI distribution showed 41.1% normal weight, 31.3% obesity, 19.6% overweight, and 8.0% underweight (Table S1).
Depression symptoms: Cases exhibited substantially higher depression symptoms across all PHQ-9 domains compared to controls (p<0.0001). The most prevalent symptoms among cases were loss of interest/pleasure (76.8% nearly every day), depressed mood (66.1%), and sleep disturbances (41.1%). Suicidal ideation was reported by 10.7% of cases versus 1.8% of controls (Table S2). Mean PHQ-9 scores were 8.75±2.06 for cases versus 0.14±0.35 for controls (Table S3).
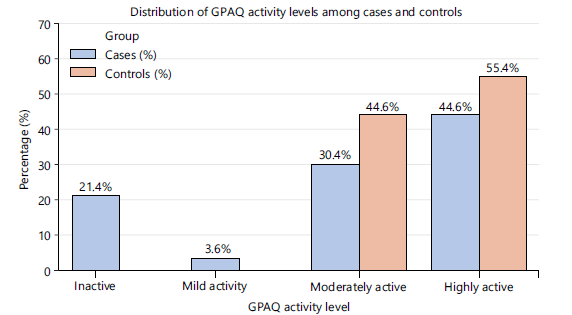
Physical activity levels: Physical activity levels assessed via GPAQ showed that cases had 21.4% inactive, 3.6% mildly active, 30.4% moderately active, and 44.6% highly active participants. Controls had no inactive or mildly active participants, 44.6% moderately active, and 55.4% highly active. Overall, cases demonstrated lower activity levels than controls. The mean METs/week was 781.28±489.11 for cases and 1048.64±377.81 for controls, with the difference being statistically significant (p = 0.003) Fig. 2.
|
| Table 1: | Bivariate analysis of socio-demographic and lifestyle factors associated with depression (n = 112) at Central Military Hospital, Poonch, Azad Jammu and Kashmir | |||
| Variable | Category/ Measure |
Cases n (%)/ Mean±SD |
Controls n (%)/ Mean±SD |
χ2/t | p-value | Crude OR (95% CI) |
| Age (years) | ≤30 | 39 (69.6) | 48 (85.7) | 4.17 | 0.041* | 0.38 (0.15-0.98) |
| >30 | 17 (30.4) | 08 (14.3) | Reference | |||
| Gender | Male | 26 (46.4) | 29 (51.8) | 0.32 | 0.571 | 0.81 (0.38-1.69) |
| Female | 30 (53.6) | 27 (48.2) | Reference | |||
| Education | Diploma Holder | 27(48.2) | 22(39.3) | 0.91 | 0.341 | 1.14 (0.68-3.04) |
| Other Degrees | 29(51.8) | 34(60.7) | Reference | |||
| Marital status | Married | 34 (60.7) | 29 (51.8) | 0.91 | 0.341 | 1.44 (0.68-3.04) |
| Unmarried | 22 (39.3) | 27 (48.2) | Reference | |||
| Income (PKR) | ≤35 000 | 29 (51.8) | 25 (44.6) | 0.57 | 0.449 | 1.33 (0.63-2.80) |
| >35 000 | 27 (48.2) | 31 (55.4) | Reference | |||
| Residence | Urban | 28 (50.0) | 40 (71.4) | 5.39 | 0.02* | 2.5 (1.14-5.46) |
| Rural | 28 (50.0) | 16 (28.6) | Reference | |||
| Job type | Private | 31 (55.4) | 25 (44.6) | 1.29 | 0.257 | 1.54 (0.73-3.24) |
| Others | 25 (44.6) | 31 (55.4) | Reference | |||
| Working hours/day | ≤8 | 29 (51.8) | 35 (62.5) | 1.31 | 0.252 | 0.64 (0.30-1.37) |
| >8 | 27 (48.2) | 21 (37.5) | Reference | |||
| BMI status | Abnormal | 31 (55.4) | 35 (62.5) | 0.59 | 0.442 | 0.74 (0.35-1.58) |
| Normal | 25 (44.6) | 21 (37.5) | Reference | |||
| Physical activity | METs/week | 781.28±489.11 | 1048.64±377.81 | t = -3.09 | 0.003* | 0.861 |
| (GPAQ) | (continuous) | (0.773-0.949) | ||||
| n: Number of participants, SD: Standard deviation, χ2: Chi-square test, t: Independent samples t-test, OR: Odds ratio, CI: Confidence interval, GPAQ: Global Physical Activity Questionnaire, METs: Metabolic equivalent task minutes per week and Reference: Category used as the baseline for odds ratio calculation. p≤0.05 indicates statistical significance (*). Continuous variables (age, GPAQ METs/week) are presented as mean±SD and analyzed using t-test, Categorical variables are presented as frequency (%) and analyzed using Chi-square test | ||||||
| Table 2: | Multivariable logistic regression analysis of factors associated with depression (n = 112) at Central Military Hospital, Poonch, Azad Jammu and Kashmir | |||
| Predictors | Response category | Odds ratio | CI (2.5-97.5%) | p-value |
| Residence | Urban | 2.66 | 1.03-8.78 | 0.019 |
| Rural | Reference | |||
| GPAQ | Continuous | 0.998 | 0.997-0.999 | 0.003 |
| R2 Tjur | 0.097 | |||
| p<0.05 considered statistically significant, CI = Confidence Interval | ||||
Association of socio-demographic and lifestyle factors with case control status: Age, residence, and GPAQ showed significant associations with depression in bivariate analysis. Adults >30 years had lower odds of depression (OR = 0.382, 95% CI: 0.149-0.979) compared to younger participants. Urban residents had higher depression odds (OR = 2.500, 95% CI: 1.140-5.460) than rural residents. Physical activity levels were significantly lower in cases (mean METs/week: 781.28±489.11) compared to controls (1048.64±377.81) (p = 0.003). Each unit increase in METs/week was associated with a 13.9% reduction in the odds of depression (OR=0.861, 95% CI: 0.773-0.949). Gender, marital status, education, income, job type, working hours, and BMI status showed no significant associations with depression (Table 1).
In the multivariable logistic regression model (Table 2), urban residence (AOR = 2.66, 95% CI: 1.03-8.78, p = 0.019) and higher physical activity levels (GPAQ METs/week) (AOR = 0.998, 95% CI: 0.997-0.999, p = 0.003) were significant predictors of depression. The model explained 9.7% of the variance (Tjur’s R2). Notably, higher physical activity was associated with lower odds of depression, while urban residence was associated with higher odds of depression in the adjusted model. Age, which was significant in bivariate analysis, was not retained in the final multivariable model.
DISCUSSION
The present study reinforces and expands on the evidence that both urban residence and lower physical activity (PA) levels are independently associated with higher depression risk among adults in Poonch, AJK. These findings are consistent with, but also nuanced by, recent global and regional research.
Recent meta-analyses and large-scale studies confirm that urban residence is often linked to higher depression prevalence, particularly in developed countries and increasingly in rapidly urbanizing regions of Asia. For example, a 2023 meta-analysis found urban residents had significantly higher odds of depression than rural residents in developed countries, though this pattern is less consistent in developing countries, where contextual factors such as social cohesion and access to services may differ11-13. In South Korea, urban residents now show higher depression rates than rural residents, a reversal from earlier years, likely due to urban stressors such as social isolation, environmental pollution, and changing lifestyles12. However, some studies in India and China report higher depression rates in rural areas, often attributed to socioeconomic disadvantage and limited healthcare access, highlighting the importance of local context14,15.
The protective effect of physical activity against depression is robust and well-documented across diverse populations and study designs. Large meta-analyses and umbrella reviews consistently show that higher PA levels, especially moderate-to-vigorous activity, are associated with significantly reduced odds of depression, regardless of age, gender, or region5,16-20. Even low-to-moderate intensity PA confers substantial benefits, and the effect is observed in both cross-sectional and longitudinal studies5,17,19. Biological mechanisms include increased BDNF expression, anti-inflammatory effects, and improved neuroplasticity, while psychosocial mechanisms involve enhanced social support and reduced loneliness, particularly when PA is group-based21,22.
The urban-rural depression gap may be mediated by differences in physical health, social participation, and environmental exposures. In China, urban-rural disparities in depression among older adults are partly explained by differences in physical health and self-reported health status23. In urban settings, lack of green space, noise, and social fragmentation are key stressors, while rural areas may offer protective social networks but also face unique challenges such as poverty and healthcare barriers12,13,15. The loss of age significance in multivariable models, as seen in this study, is echoed in recent research showing that the relationship between age and depression is often mediated by PA and social engagement23.
While obesity rates are high in this sample, the association between BMI and depression remains inconsistent across studies and populations. Some research finds no significant link, especially in South Asian populations, while others report a U-shaped relationship or associations modified by gender and cultural factors12,24.
This study’s strengths include its focus on an underrepresented region of Poonch, the use of validated tools, and comprehensive confounder adjustment. However, limitations such as single-center design, self-reported PA, and the cross-sectional nature of the data are common in the field and underscore the need for longitudinal, multi-site studies to confirm these findings and explore temporal relationships. using objective PA measures and biomarker assessments5,16. Future research should incorporate objective PA measures (e.g., accelerometers) and the integration of biomarkers to investigate underlying biological mechanisms. Furthermore, we encourage research into the specific urban stressors, cultural attitudes toward PA, and tailored interventions in conflict-affected or low-resource regions. Such research is vital for closing the treatment gap in Pakistan and informing policy focused on activity-friendly urban environments, integrating mental and physical health services16,17.
CONCLUSION
This study adds to a growing body of evidence that urban residence and low physical activity are key, modifiable risk factors for depression. Effective prevention in conflict-affected and rapidly urbanizing regions requires concrete, multi-sectoral actions, including the promotion of community-based physical activity programs and the integration of mental health screening into primary healthcare. Furthermore, policy recommendations should prioritize creating activity-friendly urban infrastructure, such as safe public parks and walkable pathways, to address the environmental determinants of mental health. Implementing these context-sensitive strategies is essential for closing the treatment gap and reducing the high depression burden in Pakistan.
SIGNIFICANCE STATEMENT
This study highlights that urban living increases depression risk, while higher physical activity offers protective benefits among adults in Poonch, AJK. Identifying socio-demographic and lifestyle factors associated with depression underscores the need for targeted public health strategies. Promoting physical activity and addressing urban stressors can help prevent depression, guiding policymakers and healthcare providers in designing effective, context-specific interventions.
REFERENCES
- WHO, 2025. Depressive Disorder (Depression). World Health Oid="2364160_ja"rganization, Geneva, Switzerland.
- Kandola, A., G. Ashdown-Franks, J. Hendrikse, C.M. Sabiston and B. Stubbs, 2019. Physical activity and depression: Towards understanding the antidepressant mechanisms of physical activity. Neurosci. Biobehav. Rev., 107: 525-539.
- Sieniawska, D., J. Sieniawska and P. Proszowska, 2024. The impact of physical activity on depression treatment: A literature review. Qual. Sport, 16.
- Schuch, F.B., D. Vancampfort, J. Firth, S. Rosenbaum and P.B. Ward et al., 2018. Physical activity and incident depression: A meta-analysis of prospective cohort studies. Am. J. Psychiatry, 175: 631-648.
- Dishman, R.K., C.P. McDowell and M.P. Herring, 2021. Customary physical activity and odds of depression: A systematic review and meta-analysis of 111 prospective cohort studies. Br. J. Sports Med., 55: 926-934.
- Bourke, M., R.K. Patten, L. Klamert, B. Klepac, S. Dash and M.C. Pascoe, 2022. The acute affective response to physical activity in people with depression: A meta-analysis. J. Affective Disord., 311: 353-363.
- Matias, T.S., M.V.V. Lopes, B.G.G. da Costa, K.S. Silva and F.B. Schuch, 2022. Relationship between types of physical activity and depression among 88,522 adults. J. Affective Disord., 297: 415-420.
- Wang, Z., B. Jiang, X. Wang, Z. Li, D. Wang, H. Xue and D. Wang, 2023. Relationship between physical activity and individual mental health after traumatic events: a systematic review. Eur. J. Psychotraumatology, 14.
- Choi, K.W., C.Y. Chen, M.B. Stein, Y.C. Klimentidis, M.J. Wang, K.C. Koenen and J.W. Smoller, 2019. Assessment of bidirectional relationships between physical activity and depression among adults. JAMA Psychiatry, 76: 399-408.
- WHO, 2021. Global Physical Activity Questionnaire (GPAQ). World Health Organization, Geneva, Switzerland, Pages: 22.
- Xu, C., L. Miao, D. Turner and R. deRubeis, 2023. Urbanicity and depression: A global meta-analysis. J. Affective Disord., 340: 299-311.
- Kang, S.J., J. Hwang, D. Kim and B. Kim, 2024. Regional differences in the effects of healthy aging on depressive symptoms: A Korean longitudinal study of aging (2006-2020). Front. Public Health, 12.
- Sampson, L., C.K. Ettman and S. Galea, 2020. Urbanization, urbanicity, and depression: A review of the recent global literature. Curr. Opin. Psychiatry, 33: 233-244.
- Rai, P., P. Sahadevan, T.G. Issac and J.S. Sundarakumar, 2024. Decomposing rural-urban differences in depression prevalence: A cross-sectional analysis of two community-based Southern Indian cohorts. BMJ Public Health, 2.
- Hong, C., X. Xiong, J. Li, X. Ning and D. Qi et al., 2022. Urbanization and depressive symptoms among middle-aged and older adults in China. Front. Public Health, 10.
- Singh, B., T. Olds, R. Curtis, D. Dumuid and R. Virgara et al., 2023. Effectiveness of physical activity interventions for improving depression, anxiety and distress: An overview of systematic reviews. Br. J.Sports Med., 57: 1203-1209.
- Rahmati, M., S. Lee, D.K. Yon, S.W. Lee and R. Udeh et al., 2024. Physical activity and prevention of mental health complications: An umbrella review. Neurosci. Biobehav. Rev., 2024.
- Meng, Y., N. Ma, Y. Shi, N. Zhang, J. Wu, X. Cui and W. Niu, 2024. The association of physical activity and sedentary behavior with depression in US adults: NHANES 2007-2018. Front. Public Health, 12.
- Marques, A., J. Bordado, M. Peralta, E.R. Gouveia, R. Tesler, Y. Demetriou and D.G. Baya, 2020. Cross-sectional and prospective relationship between physical activity and depression symptoms. Sci. Rep., 10.
- de Lima Queiroga, L., O. Kaufmann, R.M. Ritti-Dias, P.M. da Cunha, C.A. Minanni, R.M. Pitta and N. Wolosker, 2025. Physical activity levels are associated with depressive symptoms: A cross-sectional study of 58,445 adults. J. Affective Disord., 369: 298-302.
- Sousa, R.A.L.D., I. Rocha-Dias, L.R.S. de Oliveira, A.C. Improta-Caria, R.S. Monteiro-Junior and R.C. Cassilhas, 2021. Molecular mechanisms of physical exercise on depression in the elderly: a systematic review. Mol. Biol. Rep., 48: 3853-3862.
- Stevens, M., J. Lieschke, T. Cruwys, D. Cárdenas, M.J. Platow and K.J. Reynolds, 2021. Better together: How group-based physical activity protects against depression. Social Sci. Med., 286.
- Yang, J., X. Zheng, Y. Wang, H. Wang and G. Song, 2025. Age disparities in the association between leisure-time physical activity and depression among American adults. J. Clin. Psychol., 81: 706-714.
- Insan, N., E. Slack, N. Heslehurst and J. Rankin, 2020. Antenatal depression and anxiety and early pregnancy BMI among White British and South Asian women: Retrospective analysis of data from the Born in Bradford cohort. BMC Pregnancy Childbirth, 20.
Supplementary Data
| Table S1: | Socio-demographic and lifestyle characteristics of study participants (n = 112) | |||
| Variable | Total (n = 112) n (%) | Cases (n = 56) n (%) | Controls (n = 56) n (%) |
| Age (years) | |||
| Mean±SD | 26.72±5.36 | - | - |
| ≤30 years | 87 (77.7%) | 39 (69.6%) | 48 (85.7%) |
| >30 years | 25 (22.3%) | 17 (30.4%) | 8 (14.3%) |
| Gender | |||
| Male | 55 (49.1%) | 26 (46.4%) | 29 (51.8%) |
| Female | 57 (50.9%) | 30 (53.6%) | 27 (48.2%) |
| Marital status | |||
| Single | 49 (43.8%) | 22 (39.3%) | 27 (48.2%) |
| Married | 63 (56.3%) | 34 (60.7%) | 29 (51.8%) |
| Highest education | |||
| High school | 34 (30.4%) | - | - |
| Diploma | 51 (45.5%) | 26 (46.4%) | 29 (51.8%) |
| Undergraduate | 17 (15.2%) | - | - |
| Postgraduate | 10 (8.9%) | - | - |
| Socio-economic status | |||
| Low | 38 (33.9%) | - | - |
| Middle | 66 (58.9%) | - | - |
| High | 8 (7.2%) | - | - |
| Family income (PKR) | |||
| Mean±SD | 37,974±10,913 | - | - |
| ≤35,000 | 54 (48.2%) | 29 (51.8%) | 25 (44.6%) |
| >35,000 | 58 (51.8%) | 27 (48.2%) | 31 (55.4%) |
| Employment status | |||
| Government sector | 25 (22.3%) | - | - |
| Private sector | 56 (50.0%) | 31 (55.4%) | 25 (44.6%) |
| Self-employed | 22 (19.6%) | - | - |
| Unemployed | 9 (8.0%) | - | - |
| Residence | |||
| Rural | 44 (39.3%) | 28 (50.0%) | 16 (28.6%) |
| Urban | 57 (50.9%) | 28 (50.0%) | 40 (71.4%) |
| Semi-urban | 11 (9.8%) | - | - |
| Dietary pattern | |||
| Home-made | 52 (46.4%) | - | - |
| Fast food | 49 (43.8%) | - | - |
| Outside | 11 (9.8%) | - | - |
| Working hours per day | |||
| ≤8 hours | 64 (57.1%) | 29 (51.8%) | 35 (62.5%) |
| >8 hours | 48 (42.9%) | 27 (48.2%) | 21 (37.5%) |
| Body mass index (kg/m2) | |||
| Mean±SD | 24.12±4.10 | - | - |
| Underweight | 9 (8.0%) | - | - |
| Normal weight | 46 (41.1%) | 25 (44.6%) | 21 (37.5%) |
| Overweight | 22 (19.6%) | - | - |
| Obese | 35 (31.3%) | 31 (55.4%) | 35 (62.5%) |
| Physical activity (GPAQ) | |||
| Mean METs/week±SD | 914.96±455.30 | 781.28±489.11 | 1048.64±377.81 |
| Inactive | 12 (10.7%) | 12 (21.4%) | 0 (0.0%) |
| Light activity | 2 (1.8%) | 2 (3.6%) | 0 (0.0%) |
| Moderate activity | 42 (37.5%) | 17 (30.4%) | 25 (44.6%) |
| Highly active | 56 (50.0%) | 25 (44.6%) | 31 (55.4%) |
| -: Not reported separately by group in the original analysis, GPAQ: Global Physical Activity Questionnaire, METs: Metabolic equivalent of task and PKR: Pakistani rupees | |||
| Table S2: | PHQ-9 symptom-level frequency distribution among cases and controls | |||
| Cases (n = 56) - n (%) | Controls (n = 56) - n (%) | |||||
| PHQ-9 Item | Not at all | Several days | >Half days | Nearly every day | Not at all | Several days |
| 1. Little interest or pleasure in doing things |
12 (21.4%) | 0 (0.0%) | 1 (1.8%) | 43 (76.8%) | 56 (100%) | 0 (0.0%) |
| 2. Feeling down, depressed, or hopeless |
15 (26.8%) | 0 (0.0%) | 4 (7.1%) | 37 (66.1%) | 55 (98.2%) | 1 (1.8%) |
| 3. Trouble falling or staying asleep, or sleeping too much |
29 (51.8%) | 1 (1.8%) | 3 (5.4%) | 23 (41.1%) | 55 (98.2%) | 1 (1.8%) |
| 4. Feeling tired or having little energy | 38 (67.9%) | 5 (8.9%) | 5 (8.9%) | 8 (14.3%) | 55 (98.2%) | 1 (1.8%) |
| 5. Poor appetite or overeating | 38 (67.9%) | 2 (3.6%) | 10 (17.9%) | 6 (10.7%) | 53 (94.6%) | 3 (5.4%) |
| 6. Feeling bad about yourself or letting others down |
41 (73.2%) | 2 (3.6%) | 11 (19.6%) | 2 (3.6%) | 56 (100%) | 0 (0.0%) |
| 7. Trouble concentrating on things | 46 (82.2%) | 4 (7.1%) | 1 (1.8%) | 5 (8.9%) | 55 (98.2%) | 1 (1.8%) |
| 8. Moving or speaking so slowly that others noticed |
50 (89.3%) | 3 (5.4%) | 2 (3.6%) | 1 (1.8%) | 56 (100%) | 0 (0.0%) |
| 9. Thoughts of being better off dead or hurting yourself |
47 (83.9%) | 0 (0.0%) | 3 (5.4%) | 6 (10.7%) | 55 (98.2%) | 1 (1.8%) |
| Values expressed as n (%). Bold text cells indicate ≥10% of cases reporting symptoms nearly every day. Controls reported near-zero symptom burden across all items | ||||||
| Table S3: | Mean PHQ-9 score and physical activity level by study group | |||
| Measure | Cases (n = 56) Mean±SD | Controls (n = 56) Mean±SD | p-value |
| PHQ-9 total score | 8.75±2.06 | 0.14±0.35 | <0.0001 |
| Physical activity (METs/week) | 781.28±489.11 | 1048.64±377.81 | 0.002 |
| *Statistically significant (p<0.05), PHQ-9: Patient Health Questionnaire-9 and METs: Metabolic equivalent of task, Mean differences were tested using an independent samples t-test | |||
How to Cite this paper?
APA-7 Style
Ashraf,
W., Batool,
S.A. (2026). Effects of Physical Activity on Depression Among Adults: A Case-Control Study. Asian Science Bulletin, 4(2), 43-53. https://doi.org/10.21124/asb.2026.43.53
ACS Style
Ashraf,
W.; Batool,
S.A. Effects of Physical Activity on Depression Among Adults: A Case-Control Study. Asian Sci. Bul 2026, 4, 43-53. https://doi.org/10.21124/asb.2026.43.53
AMA Style
Ashraf
W, Batool
SA. Effects of Physical Activity on Depression Among Adults: A Case-Control Study. Asian Science Bulletin. 2026; 4(2): 43-53. https://doi.org/10.21124/asb.2026.43.53
Chicago/Turabian Style
Ashraf, Waseela, and Syeda Amina Batool.
2026. "Effects of Physical Activity on Depression Among Adults: A Case-Control Study" Asian Science Bulletin 4, no. 2: 43-53. https://doi.org/10.21124/asb.2026.43.53

This work is licensed under a Creative Commons Attribution 4.0 International License.